Introduction
Endoscopic surgery is the buzzword among patients who have to undergo surgery these days. Such surgical procedures are also referred to as minimally invasive surgery or keyhole surgeries. “While the term is pretty vague, ‘minimally invasive’ – or endoscopic or ‘keyhole’ surgery – generally means operations that are less traumatic than traditional surgery.” (Griffin, 2008). There is a general perception among patients and their relatives that endoscopic surgery is better when compared with traditional surgery. Whether it is true or not, such enthusiasm has resulted in the extensive use of this method for operations by hospitals and doctors alike. This trend, while it may sound good for the patients, is not always welcome to the doctors who perform such operations. The main difficulty of endoscopic surgery as far as surgeons are concerned is the use of surgical tools. This paper deals with the development of forceps used in endoscopic surgery, its limitation and, if possible, suggesting a new design that is more flexible and easier to use. If designing such forceps is possible, a comparison with existing tools will also be made.
Conventional surgery
According to medical experts, there is not much difference, as far as the treatment goes, between conventional surgery and endoscopic surgery. The main advantages of endoscopic surgery are that it gives the patient very little post-operative trauma. Conventional surgery entails a crude opening of the body. This means that the patient will need more post-operative care and time to recuperate. In traditional surgery, scars will last for a long time. But endoscopic surgery is more strenuous on the surgeon operating. Such a surgery takes much longer to complete and the surgeon needs to develop additional skills. In cases where the patient is very unhealthy, and the operation needs a long time to be performed, conventional surgery is preferred to endoscopic surgery. Moreover, even though endoscopic surgery is gaining in popularity, it has not reached a stage where all operations on the human body can be done this way.
Endoscopic surgery
Since this topic deals with the practical tools used for endoscopic surgery, a little discussion on what endoscopy is, and why designing tools like forceps is difficult, is in order. Endoscopy is a surgical procedure carried out through small incisions or openings in the body. A tube, with a miniature camera and light fixed at the end, is inserted into the body. Specially designed tools that fit in through this opening or other simultaneous small openings are used to perform what is required for the operation. “Refinement in fiber optic technology and engineering has produced instruments which are used for so-called ‘keyhole’ surgery. Fine tools can be passed into the abdominal and chest cavities so that many operations which previously required major incisions can now be performed through quite small puncture wounds.” (Dictionary: Surgery: Minimal access Surgery. 2008). An open wound where the surgeon can see what is happening with space to do the operation does not occur in this case. Surgeons have limited vision, coupled with additional distance to the operating site. Moreover, the specially designed tools are awkwardly shaped and delicate movements required in an operation are hampered.
Apart from visual and perception problems, the surgeon faces the problem of moving the tools inside the body due to the inherent design of the tools. All endoscopic tools are long and unwieldy. In open surgery with forceps of optimal length and relatively straight shape, the surgeon can feel how much pressure can be applied in using the forceps. With long forceps such as those used in endoscopy, the surgeon will have to hold his hand high about the point where the forceps are to be applied. Long periods of using this position will cause exhaustion to the arm. An overly long tool also will not give the feeling of correct pressure to be used. One way to ease this problem is to select an incision point that will give an ideal relationship between the point to be operated on and the length of the forceps. But this is not feasible in all cases and hence the problem remains as it is.
Development of endoscopic forceps
Miniature forceps
In this age of miniaturization, research has been conducted on reducing the size of components and products around the world. This is especially true in the field of medicine. Forceps using this technology have been developed. Forceps have joints that are a potential hazard for hygiene. Microorganisms can get collected in such joints which can cause potential health hazards if such contaminated instruments are used inside the body. “However, extremely small and joint-free instruments can be generated using novel materials based on various biocompatible alloys of nickel-titanium alloys (NiTi).2 Because of the superelasticity of NiTi, strains of up to 8% can be achieved in certain temperature ranges under the influence of a deformation force; following relief, these materials return to their initial state.” (Guber, 2008).
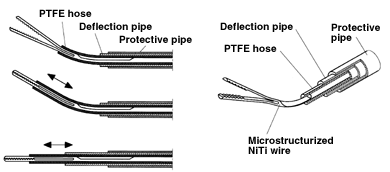
Functioning principle of a joint-free micro-instrument made of NiTi. The distal end of the micro-forceps can be deflected continuously in the range of 0° to 40°. (Guber, 2008). A PTFE hose is used to open and close the forceps. The forceps can be closed by extending the hose and it can be opened by retraction of the hose.
Endoscopic forceps that provide tactile information
Tactile information means something related to the sense of touch. As mentioned earlier, sense of touch when using the instrument is difficult during Endoscopic surgery. The research and development department of a company called Dornier has developed such a forceps for getting tactile information. The experiment using this instrument has been done for testing of tumours inside the colon. Miniature sensors have been fixed in these forceps which will provide tactile information on the surgeon’s monitors. A picture of the device is given below:
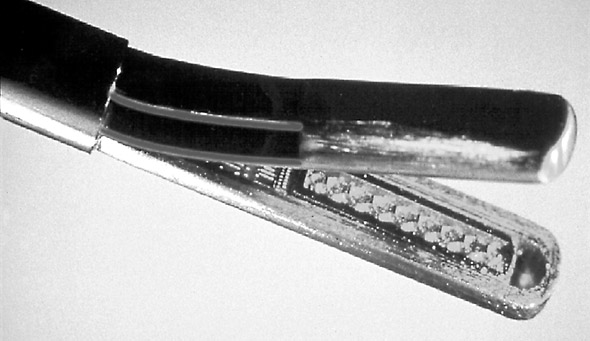
“In experimental work, we have been successful in graphically demonstrating the tactile information on the monitor; however, the microstructure sensors do not provide reliable and reproducible information, so use in the clinical routine is still not possible.” (Buess 2000).
Flexible forceps
Flexible forceps are available mainly for performing biopsies. It simply means that such forceps are flexible and hence very useful for performing functions inside the body through a tube used in endoscopy. “Flexible nephroscopy helps inspect all calyces carefully, and small calculi found therein can either be removed with the flexible forceps/tipless stone basket, or flushed out into the main system for removal.” (Rai). Another advantage of flexible forceps is that they can be used to grip objects firmly. “Flexible endoscopy forceps provide a very firm grip and with a Teflon sleeve they can be negotiated around curves.” (Shah 1982).
Grasping forceps
These types of forceps are used in endoscopy to grasp and then push or pull matters such as lesions and tumours for the purpose of easing surgical procedures. “Once a gastric foreign body is located and grasped by one of the devices (snare, basket, or forceps), it is drawn back in contact with the tip of the endoscope.” (Bounds 2006). As new technologies such as nanotechnology develops, its spin-off can benefit medical science also. When nanotechnology matures to its full bloom, scientists may invent forceps that are so small that the whole device can be inserted through the endoscopy tool. Miniature machines, also inserted inside the body through the endoscopy tube, will be operated by the surgeon with the help of a high definition TV. Such rich pictures will help identify even small and difficult to distinguish abnormalities inside the human body.
Bibliography
BOUNDS, Brenna C (MD) (2006). Endoscopic Retrieval Devices: Latex Protector Hood: Device Operation. Techniques in Gastrointestinal Endoscopy. Elsevier. P.16. Web.
BUESS, Gerhard F (2000). Robotics and Allied Technology in Endoscopic Surgery: Tactile Information. Arch Surg 2000. Archives of Surgery. Web.
Dictionary: Surgery: Minimal access Surgery. (2008). Anwers.com, Health. Web.
GRIFFIN, R. Morgan (2008). Surgery Lite: Understanding Endoscopic Surgery: When is Minimally Invasive Surgery Better than Traditional Surgery? What are the Risks? Web MD, Better Information Better Health. Web.
GUBER, Andreas E (2008). Micro Instruments for Endoscopic Procedures. Medical Device Link, The Online Information Source for the medical device industry. Web.
RAI, Samir. Flexible Endoscopy in Urology: Nephroscopy: Caculi. Bombay Hospital Journal, Issue special. Web.
SHAH, T. R (1982). Removal of Embolised Catheters Using Flexible Endoscopy Forceps. [online]. British Heart Journal, Heart, Pub Med Central. 48(5). P. 497-500. Web.