Introduction
The idea that addiction is genetic has been argued for some time in the medical and scientific communities. Proponents of this theory place much emphasis on heredity and a specific gene in the family tree that could be identified as the cause of a person’s propensity for addictive behavior. It is presumed that recognizing genetic traits will help differentiate a variety of clinical conditions associated with addictive behaviors that have often been obdurate. Others believe that addiction and addictive behaviors are somehow a moral reflection of a person’s poor choices. Many believe that addiction reflects a person’s laziness, lack of good character, and/or immorality. In researching a person’s genetic predisposition to addictive behaviors, one will find that many arguments can be made for each of the above-mentioned opinions and beliefs in the medical and scientific communities.
The popular diagnosis bio-psychosocial model of addiction treatment is intended to consider genetics (heredity), environment and social settings to determine the appropriate treatment plan for those with addictive disorders. The following will explore the specific gene theory, in particular, the D2R2 gene and the A1 variation identified in persons with addictive behavior and its subsequent effect on the “reward” portion of the brain and the chemicals of dopamine and serotonin, or deficiencies of the same. Additionally, exploration of a person’s family, medical, emotional, social and environmental history, may provide a clearer insight into the overall picture of one’s propensity to engage in addictive behaviors. The basis of this research will be that no one gene causes addictive behavior but rather heredity (genetics) in combination with the psychosocial realities of an individual, certainly influencing the chances of a person to become addicted to a substance or self-destructive behavior.
Genetics
Genetics is a very important part of the study of addictions. Since the formation of human behavior is influenced by a multitude of genetic traits and environmental influences, recent studies on psychology and human behavior depend more on genomic studies. Studies reveal that though there is no single gene for addictive behavior, heritability for alcoholism, drug dependence, smoking, and ‘novelty-seeking’ are “genetically comorbid” and each disorder has “distinct, independent genetic influences” (Lende & Smith, (nd)). When scientists look for “addictive genes”, they look for biological differences that make one person more or less vulnerable than another person to addictive behavior. People with certain genetic makeup may find it hard to quit using addictive substances once they start. Other genetic factors may prohibit a person from becoming addicted. Certain people may have an adverse physical reaction to a drug that makes other people feel good.One genetic makeup will never doom one to becoming an addict. Environment and other situational factors make up a large part of the addictive tendency. (Chein, 1969).
There is no single addiction gene. Addiction is viewed as a heterogeneous disease that is generally classified in behavioral terms. Literature reviews reveal that genetic and neurobiological factors are responsible for addictive incidents. ‘Novelty seeking’ is the driving force that influences individuals to seek out new experiences, even though well aware of the dangerous consequences, which is considered as the primary reason for development of addictive behavior. Research evidence suggests that both environmental and genetic influences are associated with addictive behavior. Similar to other behavioral diseases and maladaptive traits, the propensity for addiction is a complex issue. Many factors can be assessed in determining the likelihood that someone will exhibit addictive behavior or become an addict in their lifetime (Chein, 1969). Behavioralists assert that normal variations in personality characteristics, such as thrill-seeking, worry, anger, and addictive behavior are linked to genetic roots.
An individual’s susceptibility to addiction is the result of the interaction of many genes and scientists have yet to, and may never identify one single gene that correlates directly to addiction. Scientists have studied the family tree for addiction genes and the likelihood that those genes are handed down in the DNA makeup of later generations. Their conclusion was that not every addict carries the same gene and not everyone who has the gene will exhibit the trait of addiction(Falk, 1983). Genetically evolved traits are identified to help solve some individual problems of an organism, because ‘biological adaptation improves ability to grow, survive, reproduce, and ultimately ensure the reproduction and growth of offspring’ (Lende & smith. (n.d)). Nestler (2001) proposes that applying psychogenomics, using genomics and proteomics to explore biological substrates of normal and abnormal behavior, to the study of drug addiction will lead to the identification of genes and their protein products that control the reward pathways of the brain and their adaptions to drug of abuse, as well as variations in these genes that ‘confer genetic risk for addiction and related disorders.”
In the first step of trying to identify addictive genes, researchers examine DNA for a family pedigree to determine what genes are passed from a mother and father to a child. Individual behavioral distinctions for genetic variation are influenced by DNA sequence differences, because two alleles inherited from each parent may represent dissimilar base sequences of the DNA coding. Since gene expressions are regulated differently among body tissues and organs, even in different regions of the brain, there will be intricate gene structure and function. In such situations, examination of comorbidity for personality differences in monozygotic and dizygotic twins and comparable family studies are used to analyze complex traits. Even if an addictive gene is identified and passed to a subsequent generation’s DNA makeup, certain environmental factors may cancel out or add to one’s inclination to engage in addictive behavior. Genetics does play a very important role in the study of why someone becomes addicted. To say that there is one gene that causes this behavioral disease in all cases would be untrue.
Scientific efforts focused on the complex interaction of genetics and human behavior studies were scanty due to the “inherent difficulty in applying standard scientific techniques” and the “social implications of research in behavior genetics.” (Koliopoulos, 2005). It has been a matter of debate among the scientific sorority about the behavioral pattern of addiction, but developments in genetic studies are considered a vital medium to clarify addiction mysteries. Studies show that this is a very complex disease that involves genetics and environmental factors. (Genetic Science Learning Center, 2009) Some addicts can certainly trace their family pedigree along with their environment in trying to understand and treat their disease. Others are born with addictive genes yet never become addicted or exhibit addictive behavior for reasons that may be associated with their particular psychosocial life experience (Genetic Science Learning Center, (2009, March 1). More research needs to be done about genetics and addictive behavior. The more knowledge gained regarding the correlation of genes to the disease of addiction, will no doubt lead to breakthroughs for the treatment of addiction in the medical, pharmaceutical and addiction treatment professions.

Specific genes and gene disorders can play a role in a person’s propensity to become an addict (Leshner, Alan 2001)

Some of the most definitive gene research has identified a “reward” gene that many thought to be directly related to alcoholism. The first illustration in the above chart sites the DRD2 gene and the A 1 allele of that dopamine receptor gene more common to people addicted to alcohol or cocaine. It is well established that both alcohol dependence and smoking are complex behaviors that are predisposed to environmental and genetic factors. Studies indicate that there is the correlation between alcohol dependence and habitual smoking, and both are related to alterations of dopaminergic neurotransmission. Ernest Noble of UCLA and colleagues were the first to conduct genetic studies among human models, in 1990. They reported a strong association between alcoholism and one version of a gene, called A1 that responds to dopamine D2 receptor (DRD2), a chemical messenger in the brain’s ‘pleasure centre’ which is labeled as “reward” gene. Though there were opposing findings that ruled out any genetic difference between living alcoholics and non-alcoholics, supporters of Noble and team subsist their view of the “gene’s influence to a variety of compulsive disorders including cocaine addiction and obesity”. Another genetic study of Dean Hamer that declared identification of ‘gay genes,’ in 1993, created intense criticism in genetic studies. The identification of three chromosomal regions that are said to be associated with a sexual orientation by Dean Hamer is considered as an important breakthrough in identifying neuro transmitting gene codes that influence our moods. However, fewer follow-up studies were conducted on this finding, and opponents cite essential flaws in researcher’s assumption. Because ‘human sexuality is complicated, diverse, and often inconsistent,’ it is argued that associating a particular gene for homosexuality is biologically implausible. A new term ‘novelty-seeking’ gained acceptance in scientific fraternity with the publication of reports in 1996 by Israeli and U.S researchers that linked gene and ‘normal’ personality traits.
Research done by pharmacologist Kenneth Blum of the University of Texas, San Antonio and psychiatrist Ernest Tamara, professor of behavioral sciences and psychiatry and director of the Alcohol Research Center at the University of California, Los Angeles found an association between a variation in the DRD2 and alcoholism. The A1 gene variation was present in two-thirds of 35 deceased alcoholics and only present in one-fifth of deceased non-alcoholics. Blum and Tamara named this the “reward “gene, which was associated with addiction. It was reported by some that they had discovered the “alcoholism gene,” suggesting a direct relationship between specific behavior and one gene.
Researchers connected special characteristics of individuals who are more excitable, adventurous, and impulsive than others to a variant of a gene called D4DR. It is hypothesized that different mutations of a gene that influence mood may induce self-confidence and good cheer as well as anxiety, which is regulated by brain chemical serotonin. However, substantial evidence to support the finding is yet to develop and more studies are expected to test it. In addition, studies that explore biological roots of violence are also in progress, and reports from studies conducted on children in New York that linked violence with heredity, and social stereotypes also attracted criticism for using poor ethics in the study design. Since behavioral genetics encompass very sensitive issues controversies are rampant, which restrict researchers from exploring interaction of genes on human behavior.
Based on evidence, Laakso et al (2002) articulate that “the susceptibility to develop addiction is influenced by sources of reinforcement, variable neuroadaptive mechanisms, and neurochemical changes that together lead to altered homeostasis of the brain reward system.” Principal approaches used to identify genetic causes of addiction are candidate gene approach and open-ended genome-wide scans. In candidate gene approach genes and proteins concerned with pathophysiology of addiction are considered as risk factors and it is correlated to human disease. A candidate-gene approach helped assess the influence of specific genes and proteins in the regulation of reward, motivation, and cognitive functions, and is a powerful tool to “genetically dissect behavior.” Nestler (2001) urges that “advances in our understanding of the genetics and neurobiology of drug addiction will have dramatic implications for diagnosis and prevention as well” and genomics and proteomics are powerful tools to identify intricate behavior under “normal and pathological conditions”
Individuals with deficient dopamine receptors are denied the normal rewards and pleasures in life. Once they begin to feel those pleasures from the stimulation of their dopamine receptors through the use of drugs and alcohol they continue to seek that reward or good feeling with continued use until they become addicted. Noble and colleagues found that the A1 allele (the minor form) of the D2 dopamine receptor (DRD2) gene was associated with alcohol addiction (nd). Since behavioral paradigms can reflect the pathological progression of addiction it is crucial to analyze inherited motivating factors that exacerbate addictive behavior. The culmination of addiction engrosses to a series of behavioral manifestations, and responses from all drug abuse are distinguished by ‘enhanced arousal or euphorbia’
Although many studies have been conducted on the acute responses to psychostimulants, it may be said that inadequate evidence is available about the genes contributing to tolerance, sensitization, and reward. Neural circuits are found crucial for reward and compulsive drug intake rather than specific neurotransmitter systems. Since many neurotransmitter pathways of the central nervous system critical for compulsive behavior is involved in the manifestation of addiction, many individual genes contribute to the addictive state Studies indicate that “repeated administration of psychostimulants results in the initiation and intensification of the many biochemical and behavioral manifestations that ultimately lead to the addicted state” (Laasko, et al, 2002, p.214). Recent evidence prompt us to believe that not only dopamine but noradrenergic and serotonergic systems play “significant modulatory roles in determining the pharmacological and behavioral actions of psychostimulants,” which in turn points to involvement of genes that control these neurotransmitter systems. In addition, a plethora of mechanisms involving enzymes, receptors, transporters, and proteins, as well as transcription factors of the “Jun/Fos family” that involve candidate genes are associated with addiction. Number of research findings concluded that “substance abuse has at least a partial underlying genetic basis” and twin, adoptive, and family studies focusing on alcoholism also indicated “significant genetic basis for alcoholism.” (Lende, & Smith, (nd ), p.8).
Blum and Tamara consulted with David E. Comings, MD, director of the Department of Medical Genetics at City of Hope Medical Center in Duarte, California, to investigate the ability of the DRD2 to influence addictions other than alcoholism, such as cocaine addiction, obesity and compulsive gambling.
Comings found that researchers neglected to account for polygenetic disorders by discounting the dopamine D2 receptor relation to addictive behavior. Comings asserted that polygenetic disorders are caused by the additive effect of many genes acting with the environment and each of those genes has a contributing small effect on the overall situation.
“What happened with polymorphism is that some people found an association with different behaviors, especially alcoholism, and some people did not. Some people interpreted this as meaning that the gene plays no role in these conditions. “Comings went on to say that “different studies may find that the gene that one person found played a role, may not play a role in their group, but instead of meaning that the gene is uninvolved in anything, it just means that in some groups it is involved and in some groups, it is not. (Tamara, Phillips, 1998) That is why we think that you need to look at the addictive effect of multiple genes to get a true picture.
Genetics and Addictive Behavior
The development of behavioral research that is interrelated with genetics may be traced back to the early 1900s when the American scientists used Mendelian concepts of inheritance to show that many socially harmful traits are transferred via genes. The popularization of the term ‘eugenics’ meaning ‘well borne’, coined by Francis Galton, the cousin of evolution theorist Charles Darwin, gave new fillip to genetics and family trait studies in the late 19th century. Efforts of Charles B. Davenport and his colleagues to promote the philosophy of eugenics traced certain harmful behavioral tendencies to particular races, which lead to indiscriminate elimination of ‘inferior’ people through sterilization, and Nazi extermination programs. This bitter experience made most behavioral geneticists refrain from ‘making broad statements that connect particular populations to gene-based characteristics.’ (Lehrman, 2005).
\However, biological observations on behavior through twin studies were continued for more than 70 years at the University of Minnesota Centre for Twin and Adoption Research in Minneapolis. Since the results of twin studies derived from comparing shared behaviors are difficult to interpret and can be misleading the statistical interpretations attracted criticism that the explanations may not have relevance with genetics. In this context linkage analysis using DNA-based techniques is considered more specific to study genetic influences on human behavior.
Knowledge generated from classical biological, biochemical, and behavioral approaches had contributed to the development of modern genetic research. ‘Reverse genetics’ and ‘forward genetics’ are the classical genetic approaches used to assess the behavioral consequences of addiction. Beginning with a gene and tracing the origin of phenotypes that result from mutation of candidate gene is termed reverse genetics. In the case of forwarding genetics search begins from an altered phenotype and explores for the parent gene or genes responsible for that phenotypes.
A sibling/twin/adoption study of substance initiation, use, and problem use conducted by Rhee et al (2003) showed that there were “moderate to substantial genetic influence for abusive behavior.” Examination of genetic and nongenetic contributions to the age at onset of regular alcohol use, the age at diagnosis of alcohol dependence, and the transition from regular alcohol use to alcohol dependence was carried out by Liu et al (2004) among twin pairs from the Vietnam Era Twin Registry. It revealed that there is a strong heritable basis for alcohol dependence as genetic influence accounted for 49% of the variation in the age at diagnosis of alcohol dependence.
The finding of Rhee et al (2008) is that problem use is more heritable than initiation and use is in sync with earlier twin studies. The environmental influence is suggestive of peer power, accessibility of substances, and sibling interaction. Assessment of genetic and environmental factors that affect personality disorders (PD) by Kendler et al (2008) found that “several PDs had substantial disorder-specific genetic risk factors.
Preuss et al (2007) ascertain that “behavioral reinforcement and locomotor stimulation evoked by either nicotine or ethanol are both associated with the release of dopamine from mesolimbic dopaminergic terminals located in the nucleus accumbens.” (Alcohol and alcoholism, 2008). A study of a total 333 inpatients (265 males), who met the ICD10 diagnosis of alcohol dependence, using many genetic markers across D2 dopamine receptor genes and dopamine transporter variables was conducted by Preuss and colleagues (2007) to validate their hypothesis. From the study results it was observed that many “D2 receptor gene single nucleotide polymorphisms were related to both smoking -and drinking-related behaviors.” The study support similar previous study results suggesting that there exists a relationship between the dopamine system and alcohol and substance use disorders, and D2 dopamine receptor acts as promoter gene that influences both alcohol and nicotine dependence.
Researchers on Comings team studied a group of pathological gamblers and examined as many as 35 genes that might play a role in brain levels of serotonin, dopamine as well as other brain neurotransmitters. They learned that this pathological group had genetic variances, which resulted in polymorphisms. Individual genes were examined and the role each gene played in the group (Collins, 1979). The conclusion was that genes played a major role in the condition for that group.
Further examination is needed to pinpoint an individual’s level of serotonin, dopamine and neurotransmitters connection with pathological gambling compulsions. Once this can be determined, there may be pharmacological solutions such as mood stabilizers; serotonin reuptake inhibitors or a stimulant to be part of this group’s treatment therapy.
Tamara and his associates have also studied genetic background of heroin addicts. They found that the success rate of methadone treatment was directly related to the individual’s DRD2 A1 variant. Those who relapsed had four times the occurrence of the DRD2 A1 variant than those who successfully completed the program. The determination is that those who have the DRD2 A1 variant will need different pharmacological and psychosocial treatment than those who do not have this variant.
Studies using knockout mice, to locate dopamine receptors that mediate reward, showed that D1 mutant mice displayed “reduced sensitizing response to repeated cocaine administration,” but “other dopamine receptors is sufficient to preserve the reward mechanism.” (Laakso, et al, 2002, p.218). In the case of D2 receptor knock out mice it was observed that D2 reception function is “important for many natural and exogenous rewards, the high potency of cocaine to act as a reinforcer may again overcome this defect through other signaling pathways.” It derived that D1, D2, D3, or D4 dopamine receptors have been found to be essential for the rewarding effects of cocaine, and the “preservation of reward does not seem to be due to compensatory upregulation of remaining dopamine reception subtypes.” Laakso et al (2002), suggests that various study results on dopamine receptors mediating reward indicate “either the existence of redundancy in dopaminergic reward pathways or the importance of other monoamines when dopaminergic signaling is not intact.”
Research evidence shows that the mesolimbic dopamine system is affected by most drugs of abuse and there are functional variations in dopamine receptors and genes. Lende & Smith mention that “DRD2 dopamine gene appears to contribute to liability for substance abuse and significant associations have been found between genetics variants coding for specific dopamine receptor (D4DR), and novelty seeking, which is associated with substance abuse.” D2 dopamine receptor (DRD2) has been associated with pleasure, and DRD2A1 allele has been termed as the ‘award gene.” (A, Bowiratt., & M, Oscar-Berman, (n.d)). Dopamine plays a crucial role in modulating an individual’s behavior as dopamine mediates the “wanting” involved in seeking behavior, which affect a decision to adopt behavior change.
Tamara suggests that progression from genetics being attached to treatment methods that include pharmacology has been sluggish for many reasons. There are many people who do not believe in genetics and they believe the environment, peer pressure, family upbringing lead to everything in the addicts’ life. There has not been a positive reception of the genetic aspect of addictive behavior. (Tamara, Phillips, 1998).
Tamara would like to see the above-mentioned studies addressed in the treatment community. Alcoholism and drug addiction are major problems in society. Many addicts consistently fail; hurt their families and themselves. He would like to see the treatment community execute suggestions found in the research community to treatment plans for addicts (Tamara, Phillips, 1998).
Studies in the scientific community have found that the personalities of those with the DRD2 A1 variant display risk-taking behavior. One of the manifestations of this personality conduct is risk-taking with alcohol and drugs. The individuals with the DRD2 A1 variant have shown through electrophysiological studies that they are slow to react to stimuli, indicating low dopamine levels in their brain. (Theile, 1998).
Drawing evidence from rich literature and based on the results of imaging programs in drug addiction, Volmow and colleagues (2003) have developed a model that could explain the loss of control and compulsive drug intake in the addicted individual. In this model a network of four circuits in drug abuse and addiction, which receive direct innervations from DA neurons, has been proposed, such as reward, motivation, memory and learning, and control. The circuit for ‘reward’ is located in the nucleus accumbens (NAc) and the ventral palladium. Volmow and team, drawing evidence from imaging studies, hypothesize that “decrease in the number of DAD2 receptors, coupled with the decrease in DA cell activity, in the drug abusers would result in a decreased sensitivity of reward circuits to stimulation by natural reinforcers.” They conceptualize addiction as a state-initiated by the qualitatively different and larger reward value of the drug, which triggers a “series of adaptations in the reward, motivation/drive, memory, and control circuits of the brain.”
Research has been done to ascertain the connection between human development and alcohol and drug addiction. Some individuals are prone to a greater susceptibility to addiction. (Tamara, Phillips, 1998)Dr. Frank Vocci, Jr. director of the National Institute on Drug Abuse (NIDA) Division of Treatment Research and Development suggests research has found that children who suffer from anxiety, depression, post-traumatic stress disorder, or an emerging personality disorder are more prone to addiction.
Three primary brain systems that influence substance use and abuse identified by White (1996) are (1) approach behavior; (2) reward and pleasure; and (3) contextual cues relating approach and reward with drug stimuli in the environment (Lende, & Smith, (n.d)).Based on evolutionary inclination and as an environmental resource, it is argued that individuals engage in substance use more like food, to “balance neurotransmitter levels, to counteract the effects of stress, and to provide actual and perceived benefits” In the general sense individuals engage in drug use that is considered as base needs and immediate perceived benefits. That may be for pleasure, to reduce pain or stress, to enhance energy and change emotional states, and for sexual opportunities. This novelty-seeking behavior turns to addiction when an individual exceeds the individual limits of ‘self-regulation’ and ‘self-direction’ and wanting and seeking behavior for drugs is beyond control, which necessitates therapeutic intervention.
Depression may be attributed to not just one set of genes, but also multiple sets of genes. The same could be said of anxiety or one’s susceptibility to addiction or addictive behavior. Clinically, you have something that looks like the same disease but the passageway is quite different for each individual.Those with a genetic exposure to post-traumatic stress disorder are more likely to abuse alcohol or drugs when faced with an environment that mimics their genetic-environment stress recall. This theory now has scientists looking at the models of genetics, behavior, environment and pathology, according to Schacter. (Schacter, 1978)
Over time, drug and alcohol abuse deregulates an addict’s system. The physiological consequence of this prolonged abusive behavior leads to misperception of mild stressors as severe stressors. The addicts recognize that taking alcohol or drugs will mitigate that stress. The NIDA is researching medication that would eliminate the stress response that leads to drug or alcohol cravings by normalizing the addict’s deregulated system. The specific research is studying a Corticotrophin Releasing Factor (CRF) antagonist, which would bind to CRF receptors to reduce stress in the brain.
As the normal diagnosis of drug addiction is on the basis of behavior abnormalities, similar to other psychiatric disorders, there are no adequate diagnostic tools or treatment options specific to drug addiction. Based on epidemiological studies, Nestler (2001) argue that “drug addiction is a highly heritable disorder”, and there may be no exemption with “compulsive behaviors, such as to food, sex, and gambling.” Researchers are optimistic that the advancement of individualized addiction treatment will be developed through future discoveries in the field of genetics and gene sets that influence the brain and stress responses.
An appropriate and up-to-date assessment instrument is an integral part of research in order to differentiate between an invalid and noteworthy finding. At the same time the instrument should be reliable and valid for deriving decisive conclusions consistently. Semi-structured assessment for drug dependence and alcoholism (SSADDA), derived from semi-structured assessment for genetics of alcoholism, is one such instrument used in studies of genetic influence on cocaine and opioid dependence. The SSADDA provides “extensive coverage of the physical, psychological, social, and psychiatric manifestations of cocaine and opioid abuse and dependence in addition to some Axis I and Axis II disorders” (Samet et al, (n.d), p.10). This tool with questions about onset and currency of symptoms allows chronological assessment of symptom clusters, which helps in distinguishing comorbid disorders
Biopsychosocial Model and Addiction Treatment
The most recent and popular model used for addiction treatment is the bio-psychosocial model. This model examines biogenetic traits and psychosocial history to provide a comprehensive and integrated model to form an individualized treatment plan.
Debates have been ongoing between the psychiatric community, AA and the Treatment community regarding alcoholism and addiction. Some in the psychiatric community view alcoholism and addiction as the second problem with mental health disorders being the primary disease. AA and the treatment community contend that alcoholism and addiction is the primary disease that needs to be treated even though many argue that alcoholism and addiction do not meet the disease criteria since there has been no cause discovered that could be directly treated.
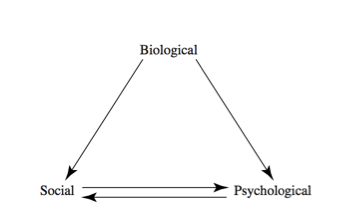
The bio-psychosocial model of addiction may be a compromise between these conflicting views. (Figure 1.3) This model is a holistic approach in that it acknowledges biological or genetic aspects impacting psychosocial aspects impacting social aspects of the individual addict in a continuing interactive manner. (Schacter, 1978)
It looks at how the person became involved in addictive behavior, how long they stay involved in addictive behavior and then stops the addictive behavior.
Winnick defines the three components of this model as: Biological includes genetic inheritance, temperament or physiological differences. Psychological factors are shared with social factors, which include interaction between the individual and family, school, work, peer and social factors. The benefit of this perspective is that it can account for difficult causative factors of addiction. This provides an individual assessment of the alcoholic or addict that measures the causes in varying amounts. One alcoholic may have no biological component yet severe depression or an abusive childhood that contributed to the alcohol abuse and ultimate addiction. (Winnick, 1962).
From a treatment perspective, many counselors consider this model a “best practices” model as it individualizes treatment plans and assists in determining when to refer out to provide the most effective and comprehensive care for an individual.
In the case of a significant genetic or inheritance component, treatment plans can include a pharmacological referral to a physician or psychiatrist to provide an assessment of brain chemistry and treatment of any deficiencies with medication.
The bio-psychosocial model of treatment remains valid because of its emphasis on all factors that contributed to the birth of an individual’s addiction and addresses those factors through the treatment plan and the use of the best available treatment along with ongoing interaction with the individual and updates and changes to the plan through a continuing collection of data and assessment.
Conclusion
There are many ongoing and definitive studies being done and concluded regarding genetic makeup and one’s vulnerability to addictive behavior. The disease of addictive behaviors is a complex one and although there has been much discovered in the way of a specific genes connection to addiction, in particular, the D2R2 A1 variance gene; there is no evidence that there is a “reward” gene that is solely responsible for addiction. Since most of the studies that support the genetic basis for addiction also support the role of environment in its comorbidity it has to be admitted that addiction is not “all genetic”–rather as a complex behavior, it reflects the impact of genes, environment, and their interaction” (Lende & Smith).
The ongoing genetic research being done to try and identify genes and gene sets that can contribute to addictive behavior is quite educational and exciting. If the treatment community was more receptive to the work of the likes of Tamara, Blum, Comings and Vocci, there is no telling what exciting breakthroughs could be made in the individual treatment of addictive behavior based on the knowledge of an individual’s genetic predisposition to the disease of addiction.
The chemical makeup of the brain could quite possibly be changed through the stimulation of certain gene receptors such as dopamine, serotonin and other neurotransmitters that may be deficient in some addicts. (1)
The physiological damage done to the addicts’ system through the ingestion of alcohol or drugs might be re-regulated to block stressors that lead to cravings for drugs and alcohol and prevent relapse.
The bio-psychosocial model of assessing treatment for an individual could be greatly enhanced with additional genetic knowledge that could be considered in the biogenetic portion of the model. Treatment professionals could refer out to physicians and psychiatrists equipped with pharmacological solutions for specific gene variances or deficiencies and quite possibly contribute to a better recovery success rate.
No one “reward” gene causes addictive behavior. Certainly, there is evidence that there are gene sets and psychosocial factors in tandem that can contribute to an individual becoming an addict.
References
- Alcohol and alcoholism: Introduction. (2008). Oxford Journals. 42(3). 258-266. Web.
- A, Bowiratt., & M, Oscar-Berman. (n.d). Relationship between dopaminergic neurotransmission, alcoholism, and reward deficiency syndrome. Cab Abstracts.
- Koliopoulos, Sophia. (2005). DNA and behavior: Is our fate in our genes: The topic in depth. The DNA Files.
- Lende, Daniel. H., & smith, E. O. (n.d). Evolution, substance use and addiction.
- Laakso, Akl., etal (2002). Experimental genetic approaches to addiction: Dopamine receptors medlating reward. Neuron. 218.
- Lehrman, Sally. (2005). DNA and behavior: Is our fate in our genes: DNA & behavior: The topic in depth: Eugenics. The DNA Files.
- Lende, Daniel. H., & smith, E. O. (n.d). Evolution, substance use and addiction: Genetic basis. 8.
- Noble, Ernest P. (n.d). Presenters. Obesity and Food Addiction Summit. Web.
- Nestler, Eric. J. (2001). Psychogenomics: Opportunities for understanding addiction: article: Identification of addiction vulnerability genes. The journal of neuroscience., 21(21), 8324-8327. Web.
- Samet, Sharon., etal. (n.d). Assessing addiction: concepts and instruments: The semi Structured Assessment for drug dependence and alcoholism. Research review assessing addiction. 10.
- Chein I. 1969. Psychological functions of drug use. In Scientific Basis of Drug Dependence, ed. Steinberg H. London: Churchill
- Collins AC. 1979. Genetics of ethanol polymerase: Role of neurotransmitters. In E. Majchrowicz (Ed.), Biochemistry and Pharmacology of ETOH. Vol 2. P. 267-221
- Falk JG. 1983. Commonalities in the environmental control of behavior. In Commonalities in Substance Abuse and Habitual Behavior, eds. Levison PK. Lexington, MA: Lexington.
- Genetic Science Learning Center (2009) Genetics is an Important Factor in Addiction. Learn. Genetics.
- Leshner, Alan I. 2001. “Addiction is a brain disease.” Issues in Science and Technology 17:75- 80.
- Marks MJ. 1983. Genetics of nicotine response in four inbred strains of mice. J. of Pharmacology and Experimental Therapeutics, P. 226, 291-302
- McHugh, M., Beckman, L., & Frieze, I. H. (1979). Analyzing alcoholism. In I. H. Frieze,
- Schacter S. 1978. Pharmacological and psychological determinants of smoking. Annals of Internal Medicine 88:104-114
- Tamara J. Phillips, et al. “Alcohol Preference and Sensitivity Are Markedly Reduced in Mice Lacking Dopamine D2 Receptors.” Nature Neuroscience 1 (1998): 610-615.
- Theile, Todd, et al. “Ethanol Consumption and Resistance Are Inversely Related to Neuropeptide Y Levels.” Nature 396 (1998): 366-369.
- Winnick C. 1962. Maturing out of narcotic addiction. Bulletin on Narcotics 14:1-7