Abstract
Catheter-associated urinary tract infections (CAUTIs) are among hospital-acquired infections, which makes their reduction in many healthcare settings a priority. Among other environments, nursing homes may experience significant rates of CAUTIs. A 100-bed unit was involved in a quality improvement project which was designed to reduce the relatively high CAUTI rates in it. Specifically, with the help of Lewin’s model, bathing with 2% chlorhexidine gluconate washcloths was implemented as a CAUTI prevention intervention. The nurses were trained to use them and provided with helpful handouts and checklists to ensure treatment adherence.
The intervention was applied to four residents for two weeks. The training was evidenced to have affected the nurses’ and nursing assistants’ CAUTI scores as measured with a self-developed instrument and the Wilcoxon signed ranks test. The state of the residents, which was assessed with dipstick urinalysis before and after the washing was implemented, did not change over the course of two weeks. The project tested a CAUTI intervention in long-term care, which resulted in statistically significant improvements in the knowledge of the nursing staff of the facility. The training may be recommended for future use.
However, the significant limitations of the project, including the fact that the recruited participants had had leukocytes in their urine before the bathing was implemented, imply that few conclusions can be made regarding the washcloths. Future research may help to contribute more data to the effectiveness of washcloths in preventing CAUTIs in nursing homes.
Nature of the Problem
Introduction to the problem
Background on the problem
In 2018, the World Health Organization (WHO) highlighted the incidences of healthcare-associated infections (HAIs). Infections can lead to lifelong disability or even death (Centers for Disease Control and Prevention, 2013). In addition, patients with HAIs spend more time in hospitals, which increases costs. Recent reports describe urinary tract infections as the fourth most prevalent form of the condition in the United States (Nicolle, 2014). CAUTIs are the most common HAIs among those; approximately 12.9% of the total health care infection relates to urinary tract infection, and 67.7% of such cases involve patients with a urinary catheter (Nicolle, 2014).
The current rates of CAUTIs in the United States (US) can be up to “4.8 per 1,000 catheter-days” (Lo et al., 2014, p. 464). CAUTIs are also very prevalent and can account for up to one-third of all infections reported by long-term healthcare institutions (Centers for Disease Control and Prevention, 2013; Nicolle, 2014). Given that 75% of CAUTI cases are evidenced to occur in long-term care facilities, the WHO deemed it necessary to implement interventions that would help resolve this issue (Centers for Disease Control and Prevention, 2013). Similarly, the Centers for Disease Control and Prevention (2017a) keep setting goals for an ongoing reduction of CAUTI rates.
Thus, multiple healthcare organizations, including US-based ones, support the need for the reduction of CAUTI rates. The daily use of disposable washcloths with 2% chlorhexidine gluconate helps reduce bacteria on the skin which can reduce the development of CAUTIs, thereby ensuring the patient’s health and general wellbeing (Amirov & Candon, 2015; Durant, 2017; Huang, Chen, Wang, & He, 2016). However, the recent investigation on the topic appears to be focused on intensive care (Huang et al., 2016). This tendency can be justified since intensive care settings are rather CAUTI-prone and may be accountable for the highest rates of CAUTIs (Lo et al., 2014).
Still, this fact means that there is a limited amount of recent research that would test the intervention in long-term care. In addition, the problem of training should be noted. Recent research suggests that nurses may require additional training to be able to address CAUTIs effectively (Jain, Thakur, Dogra, Mishra, & Loomba, 2015; Trautner et al., 2017). From this perspective, in order to effectively test the intervention, it is necessary to make sure that the staff has a sufficient understanding of the topic.
Significance of the problem in nursing and healthcare
HAIs are a crucial aspect of benchmarking when healthcare and nursing are concerned (Centers for Disease Control and Prevention, 2017a; Lo et al., 2014). The reduction of HAIs, including CAUTIs, is a goal that is commonly established for healthcare facilities and nurses in the US, as well as other countries (Centers for Disease Control and Prevention, 2017a). Given the negative outcomes of CAUTIs and HAIs, including the various complications and lethal outcomes, as well as costs associated with them (Centers for Disease Control and Prevention, 2013; Nicolle, 2014), this goal of utmost importance for healthcare and nursing.
Moreover, the issue of recent research and gaps in it needs to be considered. Evidence-based studies indicate the efficacy of using a disposable washcloth with 2% chlorhexidine gluconate as an active cleansing agent during routine care for senior patients on Foley catheter in a long-term care facility (Shippey & Malan, 2004; Delesie, Blot, Vanacker, & Vandijck, 2011; Popovich et al., 2012). The intervention is shown to decrease the incidence and prevalence of CAUTIs in different settings (Afonso, Blot, & Blot, 2016; Cao, Gong, Shan, & Gao, 2018; Strouse, 2015). In fact, the use of a chlorhexidine gluconate washcloth can significantly reduce the overall incidence of HAIs (Climo et al., 2013). In other words, the washcloths can be considered an effective solution to the problem of CAUTIs, and investigating their effectiveness in nursing homes is important.
Purpose of Project
Problem statement and purpose
The problem that was addressed by this project can be summarized as follows: CAUTIs are a type of HAIs that cause significant negative outcomes and that are prevalent in long-term care, but some of the relevant preventative measures (specifically, 2% chlorhexidine washcloths and related training) have been more extensively studied in other settings. Based on the recommendations by the Centers for Disease Control and Prevention (2017a), it is necessary to proceed to reduce CAUTI rates, which is why the application of effective, evidence-based interventions to the described settings is important.
The purpose of this two-week quality improvement project is to adapt the existing evidence for the prevention of CAUTIs in long-term care with senior patients who are over 64 years old but younger than 89. It has been established due to the identified lack of recent articles that would cover the application of chlorhexidine-impregnated washcloths in the described settings. The project focused on working to improve CAUTI rates within a particular long-term care facility (a nursing home), but in doing so, it also aimed to contribute some information on the washcloths and their applicability to nursing homes.
Thesis and PICOT question
This project does not use a hypothesis, but its thesis can be formulated as follows: based on the existing evidence, the correct usage of 2% chlorhexidine gluconate washcloths might result in care quality improvements as related to CAUTIs and their rates. In order to test this claim, a PICOT question was developed, and it was formulated as follows: for senior patients ages 65 years and above of long-term care facilities (P), how does the use of a disposable washcloth with 2% chlorhexidine gluconate (I) compared to standard catheter care (C) affect the rate and prevalence of catheter-associated urinary tract infections (O) within a two-week period (T)? This question has been used to set the project’s goal and objectives.
Project goals and objectives
As suitable for a quality improvement project, the goal of this one was to improve the ability of the project’s site, which was a unit in a nursing home, to prevent CAUTIs and reduce their rate with the help of an evidence-based intervention, which was 2% chlorhexidine gluconate washcloths. A secondary goal was to contribute the information on the applicability of this intervention to the setting of a nursing home, that is, a long-term care facility. Based on these goals, the more specific objectives included the following statements.
- Objective 1: to synthesize the evidence on CAUTI prevention with 2% chlorhexidine washcloths and ascertain that it is an evidence-based solution by the beginning of the project’s planning.
- Objective 2: to develop a methodology for the project along with the plan for data collection and its analysis and ensure that it can be carried out by approving it with the site’s personnel and Institutional Review Board by the beginning of the project.
- Objective 3: to evaluate the effectiveness of 2% chlorhexidine washcloths in CAUTI prevention in long-term care patients aged 65-89 with indwelling Foley catheters or suprapubic Foley catheters by carrying out the project over the planned two-week period.
- Objective 4: to report the results of the project.
Benefit of the project to practice
The intended benefit of this quality improvement project was a decrease in the incidence of CAUTIs within its site (a nursing home) despite the small scale of the intervention. This outcome is important for patients and their families, especially when considering the impact of CAUTI, including extended hospital stay, increased cost, lifelong disability, as well as the possibility of death (Centers for Disease Control and Prevention, 2013). Moreover, the members of the healthcare team received an opportunity to improve and practice their CAUTI prevention skills as a result of the training part of the project; their improved performance can be considered a meaningful benefit for the site. Finally, the information from this project might be employed by other facilities. Thus, the project brought some practical benefits, especially for the project’s site, and those benefits are in line with its goals.
Scope of the project
The project took place in a 100-bed nursing home unit and consisted of the implementation of a particular intervention (2% chlorhexidine gluconate washcloths) for a period of two weeks in a long-term care facility complete with staff training. The recruitment involved older patients (aged 65-89) who, by the beginning of the study, had an indwelling Foley catheter or suprapubic Foley catheter. The study was limited by its timeframe and the number of patients available. The training was used to facilitate the correct application of the intervention; all the nurses from the unit who could have been engaged in the project were involved. In a pre-test post-test quality improvement effort, the data for all the participants was collected twice; for the nurses, it consisted of CAUTI knowledge scores, and for patients, it involved urinalysis results.
Significance of the study
Healthcare practice
The project addresses an important practical issue that the nursing staff of healthcare facilities, including nursing homes, have to consider. It focuses on quality improvement, but it also produces an amount of information that may be helpful for nursing specialists who work in similar settings and with the CAUTI problem.
Healthcare outcomes
From the perspective of healthcare outcomes, the project was aimed at the reduction of HAIs (specifically, CAUTIs), which plays a part in the quality of care and patient outcomes (Lo et al., 2014). Therefore, the project is significant since it may have affected healthcare outcomes within its site, and its data can be used to do the same in other facilities.
Healthcare policy
From the perspective of healthcare policy, the project contributes some information on CAUTI prevention. These data might be helpful in developing policies related to CAUTIs and related solutions. In addition, the project investigates the effectiveness of a training program, as well as the level of CAUTI prevention preparedness in the nurses of a nursing home. Therefore, the more specific CAUTI prevention policies that are related to CAUTI training might also employ the evidence produced by this project, which makes it significant.
Summary
This paper covers a project which was dedicated to a rather significant problem that has been prevalent in multiple settings, including long-term care ones. CAUTIs were the issue that the project chose to address, and the site that it took place in was a nursing home. A literature search showed that there might have been a relative shortage of recent research dedicated to a rather effective intervention in the settings that are similar to that of a nursing home. The adjustment of this intervention to the setting became the purpose of the project. The testing of the usefulness of 2% chlorhexidine gluconate washcloths with older residents of a nursing home was significant due to its ability to improve health outcomes and produce information that might be relevant for nursing practice and policies.
Review of the Literature
In order to successfully carry out the project and achieve its objectives, it is necessary to synthesize and analyze the relevant evidence. This chapter will present some crucial information on CAUTIs and the project’s framework, but it will dedicate a lot of attention to the articles which currently suggest that the proposed intervention for the nursing home is evidence-based. Based on this information, treatment recommendations will be offered.
The Clinical Practice Problem Statement
Epidemiology
CAUTIs are the specific type of infections that occur in the urinary system and that are related to the use of catheters. They are rather prevalent; generally, they constitute about three-fourths of all the urinary tract infections, which demonstrates their significance (Centers for Disease Control and Prevention, 2013). Another factor to consider is that catheters are also rather common in healthcare; according to the Centers for Disease Control and Prevention (2013), for hospitals, at least 15% of patients receive one over the course of their stay. Thus, the specifics of CAUTIs’ determinants highlight the significance of addressing this rather frequently encountered problem.
The Centers for Disease Control and Prevention (2017a) demonstrate that since 2015, certain changes in the definition of CAUTIs were made to exclude non-infectious colonization, which led to decreases in reported CAUTI rates. As compared to the rates calculated for 2009, the 2015 rates were reduced by more than 40%. If the changes in the definitions are taken into account, at least a 17% reduction can still be observed. Over 4,000 facilities reported 27,029 instances of CAUTIs in 2015 (Centers for Disease Control and Prevention, 2017b). Furthermore, the Centers for Disease Control and Prevention (2017a) note that a decrease can be seen in the use of catheters. An increase in safer, more evidence-based catheter use approaches was also recorded. Still, the reduction in HAIs and CAUTIs remains one of the goals communicated to healthcare facilities by the Centers for Disease Control and Prevention (2017a).
Problem statement: practice situation
Based on the prevalence and negative features of CAUTIs, their reduction is a requirement for nursing settings, including the project’s site. Since its unit underperforms as compared to the rest of them within the same facility, the introduction of improved methods of CAUTI prevention is necessary. Based on the literature presented below, such a method was found and implemented as described by this practice change project.
Evaluation/Summary of the Evidence from the Literature
The collection of the evidence for the project was carried out by reviewing recent studies dedicated to CAUTI. The Walden Library Medicine, Health Sciences, and Nursing Databases were used to search for materials and references related to the clinical question regarding the effectiveness of using 2% chlorhexidine gluconate washcloths in reducing CAUTIs among patients with indwelling urinary catheters. Furthermore, the databases MEDLINE, ProQuest, and CINAHL were searched as well. The keywords included catheter-acquired urinary tract infection, CAUTI, 2% chlorhexidine gluconate, and urinary tract infection. The library and literature search returned several thousand sources, but the sample was narrowed down to seventeen recent peer-reviewed articles, which can be summarized as follows.
The evidence which indicates that the proposed solution is likely to be suitable for the task of reducing CAUTI is rather extensive. Several studies show how effective nursing management can be, especially when 2% chlorhexidine gluconate washcloths are used in caring for patients with indwelling catheters (Gefter et al., 2018; McCoy et al., 2017; Mitchell et al., 2019; Peter, Devi, & Nayak, 2018; Zurmehly, 2018). Peter et al. (2018) pointed out the primary reason for the high incidence of CAUTI, which was credited to non-sterile techniques used by nurses while handling patients with indwelling Foley catheters or suprapubic Foley catheters.
The same results were revealed in a study made by McCoy et al. (2017), which suggested that the nurse’s failure to properly handle the catheter, especially during bathing, was just one of the reasons CAUTIs occur. The bactericidal properties of chlorhexidine have also demonstrated effectiveness in reducing the incidence of surgical site infections and multi-drug-resistant organisms, such as methicillin-resistant Staphylococcus aureus and Vancomycin-resistant enterococci, by 23% when used for pre-operative bathing (Climo et al., 2013).
The relevant literature supports the idea that the use of 2% chlorhexidine gluconate washcloths during bathing could significantly reduce the rate and prevalence of CAUTI (Mitchell et al., 2019; Schmudde, Olson-Sitki, Bond, & Chamberlain, 2019; Swan et al., 2016). Below, the articles and research literature that are in agreement with this statement are presented in detail.
A study by Rhee et al. (2018) involved comparing three different types of chlorhexidine wipes with different strengths, including no-rinse 2% chlorhexidine wipes and 4% chlorhexidine liquid and cotton washcloth moistened with sterile water. This study involved 126 participants; 63 of them had one forearm cleansed with chlorhexidine 2% (Method A); 33 other participants had their contralateral arm cleansed with chlorhexidine 4% liquid (Method B); 30 participants received on one arm cotton washcloth moistened with sterile water (Method C). The authors concluded that participants who had their arm cleansed with chlorhexidine 2% had decreased microbial densities much lower than those who had the chlorhexidine 4% applied to them. In other words, the study demonstrates the effectiveness of chlorhexidine 2% at reducing microbial densities and preventing CAUTI.
The study by Sinha, Sazawal, Pradhan, Ramji, and Opiyo (2015) was a systematic review with the objective of analyzing the effectiveness of chlorhexidine on neonatal skin or cord of all newborns. The review included 12 trials (seven hospital-based and five community-based studies). The studies were done over a timeframe that ranged from six months to 37 months; the samples ranged between 112 and 29,790 individuals. According to Sinha et al. (2015), three trials with high-quality evidence found that chlorhexidine cord cleansing reduces neonatal mortality (RR 0.81, 95% CI 0.71 to 0.92), and the neonatal mortality rate reduction was 12%.
Swan et al. (2016) conducted a randomized study on 325 patients in a 24-bed surgical ICU at a quaternary academic medical center and found that chlorhexidine bath given every other day lowered the risk of infections by 44.5%. The study intended to compare daily bathing with soap and water to every other day 2% chlorhexidine wipes bathing for a period of 28 days. It was shown that chlorhexidine wipes bathing decreased the risk of HAIs (hazard ratio = 0.555; 95% Cl, 0.309-0.997; p = 0.049).
Afonso et al. (2016) presented a review and meta-analysis of 4 randomized controlled trials (n=22,850), which demonstrated the reduction of bloodstream infection and a decrease of bacteremia after the application of chlorhexidine washcloths. The goal was to measure the effect of chlorhexidine wipes on pathogens. The authors analyzed data from three different units: an intensive care unit, a pediatric care unit, and a hospital ward with and without the use of chlorhexidine wipes. The intervention led to a 64% drop in pathogen transmission.
Cao et al. (2018) discussed several randomized controlled trials and quasi-experimental trials, which considered varied approaches to urethral cleaning and compared them to disinfection with respect to their effectiveness in preventing CAUTIs. Thirty-three studies that recruited 6490 patients were included. To prevent urinary tract infection in patients with indwelling Foley catheter, different cleaning methods were used. Seven methods of urethral cleaning were deemed eligible and summarized in the network meta-analysis. Chlorhexidine wipes (2%) were the most effective solution according to the results of the Bayesian analysis; consequently, they were recommended for preventing CAUTIs.
Strouse (2015) conducted a literature search through multiple databases to find research articles on bathing and cleansing practices and CAUTI prevention. Twenty-two studies were included to demonstrate that the use of 2% chlorhexidine gluconate wipes bathing was an effective method for reducing the incidence of CAUTIs. It was found that chlorhexidine could be viewed as an antiseptic that provided protection against fungi, gram-positive and gram-negative bacteria, such as methicillin-resistant Staphylococcus aureus (MRSA), Vancomycin-resistant enterococci (VRE), and other multi-drug-resistant organisms (MDRO), as well as CLABSIS.
An article written by Wang et al. (2017) reported that the current literature suggested very strongly that chlorhexidine baths could prevent HAIs. The authors also revealed that chlorhexidine possesses a potent antibacterial reaction when in contact with gram-positive organisms. They proceeded to report the findings of a randomized controlled trial which explored the effectiveness of chlorhexidine bathing. The authors stated that chlorhexidine wipes bathing done every other day on 11 patients could save one HAI. These $33 baths could lead to saving from $6,000 to $60,000 per HAI. The authors also reported a study done by Vernon et al. (2006) (as cited in Wang et al., 2017), which revealed that chlorhexidine 2% washcloths lowered the procurement of VRE.
Carter, Reitmeier, and Goodloe (2014) presented a literature review with a study of 28-bed general/telemetry medicine unit in an Academic Health Science Center. They pointed it out that an indwelling catheter had to have been in place for a period greater than two days on the day of the event to qualify as a CAUTI. The infection was attributed to the current unit if it was greater than two days since transfer when all requirements were met.
The goals of this study included: measuring different successful interventions, including the verification of appropriate circumstances to insert an indwelling urinary catheter, the use of appropriate insertion techniques, meticulous maintenance procedures, removal at earliest possible opportunity, appropriate competency training for all relevant staff members on the new evidence-based policies and procedures for the reduction of CAUTIs.
Carter et al. (2014) carried out an analysis of the implementation of a CAUTI prevention bundle, which involved identifying standards for the insertion of catheters and standards for keeping it inserted on a day-by-day basis, developing stringent hygienic practices for the maintenance of the catheters while in use, and forming an educational campaign to teach direct-care providers, patients, and families about the proper use and hygiene of catheter. The authors reported that they used evidence-based solutions; according to them, strong evidence supported the use of chlorhexidine gluconate bathing as a means of reducing healthcare-associated infections, including central line-associated bloodstream (CLABSI) and surgical site infections (SSI).
The study demonstrated that incidence rates were reduced in a high-risk patient population implementing daily bathing with chlorhexidine non-rinse cloths. These non-rinse chlorhexidine wipes application significantly reduced the risk of colonization with vancomycin-resistant enterococcus (VRE) or MRSA. Thus, the implementation of the evidence-based CAUTI prevention bundle by Carter et al. (2014) reduced of the number of CAUTIs, improved patient outcomes, and advanced the overall standard of patient care were improved.
The Critical Care Nurse revealed that the AACN Practice Alert (2016) developed guidelines for urinary catheterization. This instrument is based on already existing tools, including the HOUDINI Protocol, and its primary aim is to standardize indwelling catheter-related assessment, providing the necessary guidance for nurses. The criteria include indications for the insertion of indwelling urinary catheters and the due application of the aseptic technique as measures that can decrease the risk factors for CAUTIs. Among other ways to prevent CAUTIs in adults, cleaning the catheter with chlorhexidine gluconate wipes was recommended as an intervention capable of decreasing CAUTI.
Certain evidence that is not fully in favor of the discussed intervention should also be referenced. Amirov and Candon (2015) reported a randomized controlled trial which compared the effects of chlorhexidine wipes and care-as-usual on methicillin-resistant Staphylococcus aureus. Over 120 patients from a chronic care hospital were enrolled, and the study lasted for 12 months. The results included a reduction in the infection rates, but its statistical significance was not demonstrated.
A recent study by Noto et al. (2015) contradicts the above-presented findings more directly. In this ten-week cross-over randomized trial, over 9,000 intensive care patients were bathed with chlorhexidine washcloths. No statistically significant HAI reductions were found. However, a more recent meta-analysis of the same intervention within the same settings by Huang et al. (2016) reached the opposite conclusion after examining fifteen recent studies, including randomized and quasi-experimental ones. In summary, most studies demonstrate HAI and CAUTI reduction associated with varied chlorhexidine interventions and in different settings, but there is some conflicting evidence.
Critical Appraisal of the Evidence
The presented articles were chosen for their high quality. The weakest article is the recommendation by AACN Practice Alert (2016), which does not provide details on its methodology. The rest of the articles support the findings of this source, however. The meta-analyses were thorough in their review of the literature and assessed the quality of their evidence; they employed all the available literature that was applicable to their specific topic. The randomized trials presented their methodology in detail; with the exception of Rhee et al. (2018), they had large samples and significant duration.
Regarding their applicability, not all presented articles were concerned with testing daily bathing in long-term care with 2% chlorhexidine washcloths. Only one article was fully focused on the settings that are associated with long-term care; it is a randomized trial that took 12 months and involved 122 patients of a chronic care hospital (Amirov & Candon, 2015). It also considered staphylococcus infections, which means that it did not reflect the same outcomes as the ones of interest to this project. In the end, no study was found with the exact combination of the settings, outcomes, and intervention that the project uses. However, on their own, the setting (Amirov & Candon, 2015), outcome (Swan et al., 2016), as well as the intervention (Huang et al., 2016; Swan et al., 2016), were studied, and evidence to the effectiveness of said intervention was found.
Presentation of Theoretical Basis
Change in any environment requires assessment, planning, and evaluation. Kurt Lewin, the author of the Change Model in Nursing, identified the three stages of change: unfreezing, change, and refreezing (Lewin, 1947; Scott, 2016). According to Lewin (1947), in order for a change to take place, it is necessary to unbalance the existing state of events (that is, the status quo) first. Thus, the first stage of the model involves determining the factors that can prevent the change (and support the status quo) and address them, for example, by changing attitudes toward the existing system. When this stage is completed, change is supposed to be carried out; this second stage is characterized by actually making progress in implementing the new feature.
Finally, when the change is sufficiently well-established, it can be refrozen, which means that it is supposed to become solidified as the status quo. This model has been criticized for simplicity, but it is also praised for its ability to structure change and focus on the factors that can hinder it (Cummings, Bridgman, & Brown, 2016). In addition, the simplicity can be viewed as a specific feature or an advantage that makes the model moldable. This project utilized the positive aspects of the model by employing most of its concepts.
Theoretical Framework’s Relationship to the Clinical Problem
The described model has been applied to the project because its introduction could help to structure the implementation of the studied intervention. Indeed, the described project was predominantly aiming to reduce CAUTIs by adopting an intervention that was likely to have positive effects. The implementation of this intervention could be considered a change, and Lewin’s (1947) model was devised specifically to guide such events. Therefore, the model is related to the clinical problem and its solution.
Indeed, using the terminology of the model, the most common bathing practice for patients with indwelling Foley catheter or suprapubic Foley catheter is limited to the use of non-chlorhexidine gluconate washcloths. However, this practice has been proven ineffective in managing and controlling the spread of CAUTI (AACN Practice Alert, 2016). Therefore, a model which instructs change agents to unfreeze the status quo fits the described quality improvement project.
Based on the model, the unfreezing stage was supposed to be considered first. During that period, which preceded the implementation of the intervention, the need to change the previously existing practice was advocated for by pointing out the incidence of CAUTI cases which compromised the health and general welfare of patients. In order to promote this process, it was necessary to establish and demonstrate the fact that the use of traditional washcloths was less effective when compared to 2% chlorhexidine gluconate washcloths.
In addition, it was brought to everyone’s attention that by institutionalizing this practice, the project’s site could avoid future problems which would be costlier and more effort-consuming. A major aspect of unfreezing was the training element of the project; the participants were taught to use the washcloths and provided with the information about it, which promoted their use.
All these factors enabled the change procedures, which consisted of introducing the new practice and monitoring the adherence of the participants to it. Constant monitoring, follow-ups, and evaluation were guaranteed with special handouts that took the form of check-lists; they were supposed to assure the effectiveness and efficiency of the practice. Once accepted, this new intervention has the potential of taking full effect; it might even be made permanent (refreezing). However, this aspect of the model was not directly implemented during the project because of its short duration. To summarize, the application of Kurt Lewin’s model to the project as its theoretical framework helped to guide its implementation, addressing the problem, and facilitating its solution within the chosen facility.
Utility/Feasibility
The proposed change was feasible and could be useful due to its potential benefits and theoretical underpinnings. Indeed, Lewin’s model can be considered an asset. Popularized and fully formed, as well as expanded upon, after Lewin, this model became a classic change management approach in various fields, including nursing (Cummings et al., 2016; Scott, 2016). For this project, it was mostly chosen because it could direct a quality improvement effort. Furthermore, the presented literature suggests that the project’s focus on CAUTIs is reasonable and that the established solution can be expected to have positive outcomes (Huang et al., 2016). No studies of the cost-effectiveness of the washcloths were found, although chlorhexidine was shown to be more cost-effective than saline (Mitchell et al., 2019). Still, given the well-pronounced practice problem, it is reasonable to test the washcloths in a nursing home both to fill the gaps in research and attempt to improve the quality of care.
Recommendations Summary
It can be established that chlorhexidine is a reasonable intervention to implement when the reduction of HAIs is necessary (Mitchell et al., 2019; Noto & Wheeler, 2015). Moreover, research indicates that bathing 2% chlorhexidine gluconate washcloths is a suitable intervention, which is especially well-evidenced for intensive care units (Huang et al., 2016). Long-term care can also benefit from this type of intervention (Amirov & Candon, 2015). From this perspective, it is possible to recommend the intervention for the project’s site.
Evidence Table
The table with the key articles that are important for the project is presented below. It has been and will be used for the evaluation of evidence in the sections above and below. The level of the presented evidence is determined with the help of the evidence pyramid as reproduced by Polit and Beck (2017). The articles include the ones related to CAUTIs and training since the project involved providing the nursing staff with the knowledge that was required for using the washcloths.
Table 1. Evidence Table.
Evaluation (All Literature)
The literature review of CAUTI prevention contains sufficient evidence which demonstrates that chlorhexidine is an effective solution. The limitations of the studies, especially their samples, which can be rather small and restricted to a particular setting, are offset by their high quality and the magnitude of the presented evidence. The review supports the use of 2% chlorhexidine washcloths to reduce CAUTI incidence in various populations, especially adults, and different settings. Therefore, the literature demonstrates that the chosen solution is evidence-based and likely to improve the quality of care for the population of interest, which consists of people at risk of developing CAUTI.
As for training, the problem of insufficient training is supported by two surveys, one of which was focused on nursing homes and had a relatively impressive sample (Trautner et al., 2017). The other one was significantly less generalizable, but it also involved nurses from the US, which makes it valuable as well (Jain et al., 2015). Since the project focuses on the implementation of a new approach to resident bathing, this information is sufficient to support the introduction of the training aspect of the intervention.
Level of Evidence
The literature that presents the evidence for the usefulness of chlorhexidine in infection prevention mostly consists of meta-analyses and randomized controlled trials, although a recommendation (guideline) of a reputable organization was included as well. Such studies offer evidence that is very reliable, and the extensively described methodologies of these articles demonstrate that they are also high-quality (Polit & Beck, 2017).
However, some of the meta-analyses referenced insufficient or insufficiently high-quality data that they had to incorporate (Sinha et al., 2015; Wang et al., 2017). The conflicting study produces evidence of a lower level when compared to meta-analyses, but it is also a very high-quality study with a large sample and duration (Noto et al., 2015). Given the above-discussed gaps in research, it can be concluded that there exists high-level evidence for the use of chlorhexidine, including its application in the form and settings of the project, although it is not fully conclusive. Regarding training, as a non-randomized study, a survey only provides IV-level evidence (Polit & Beck, 2017), but its ability to demonstrate the prevalence of issues is valuable for the project.
Outcomes and Summary
This chapter covered the literature that could help to contextualize the project’s key concepts. Thus, it further indicated the significance of the project by demonstrating the prevalence of CAUTIs, aggregated the evidence which supports the intervention of interest, and provided a general overview of the model that was employed to implement it. Based on these findings, it can be concluded that the project utilized a well-established change model to implement a sufficiently evidence-based solution to its very significant problem.
Methods
Recommendations of Practice Change
Based on the information presented in the literature review, the implementation of daily bathing with 2% chlorhexidine washcloths is recommended (Huang et al., 2016), as well as relevant training for its use (Jain et al., 2015).
Plan for implementation of EBP practice change
Overview of the approach
The methodology used for this project adopted a quantitative pre-test post-test approach to establish the effectiveness of the intervention and training associated with it. The variables included the washcloths bathing, which was independent; the CAUTI status for residents and CAUTI knowledge for the staff were the dependent variables. The urinalysis of the residents’ samples was used before and after the implementation of 2% chlorhexidine gluconate washcloths to determine the pre- and post-intervention values; leukocytes and nitrites were used for the measurements. The training intervention and its effectiveness were evaluated and tested in the same way; before the training, the CAUTI knowledge of the enrolled staff was assessed, and after the training, the procedure was repeated. The tool that measured this variable was developed for that task. The training took 30 minutes, and the bathing was carried on for two weeks. The details of the approach will be discussed below.
Project design
As stated above, the design of the project is defined by the term “pre-test post-test.” Consequently, it involves no control groups; only one sample of a particular population (in the case of the project, residents, and nurses) was studied. In both cases, an intervention was introduced after the first data collection procedures; after its termination, the process was repeated. This way, the project was supposed to determine the ability of the intervention to affect the outcomes of interest, which were expressed through the measurements of the two independent variables.
The choice of the design is explained by the fact that the PICOT looks for a relationship between the intervention and measured outcomes (CAUTIs). Since only quantitative approaches are suitable for the task (Polit & Beck, 2017), it was reasonable to choose one. As for the post-test pre-test design, it is quasi-experimental, which restricts its ability to prove the relationship that the PICOT searches. Still, Polit and Beck (2017) highlight the usefulness of this approach, especially for quality improvement projects. Since the presented project was rather significantly restricted in access to residents, an experiment could not be carried out, but a pre-test post-test methodology could be employed. Therefore, the limitations of the projects played a part in determining the suitable design, but it was predominantly chosen to respond to the PICOT.
Site, agency, and participant information
Claridge House is a 240 bed-licensed Nursing Home located in North Miami, Florida, which consists of three units (1-South, 2-South, and 1-North). The prevalence of CAUTIs in the 2-South unit with 100 beds was significantly higher than the other two units; it was used for resident recruitment. The project supported the facility’s goal, which includes the topics of increasing resident safety and satisfaction, preventing money loss associated with CAUTIs, and avoiding penalties imposed by the Centers for Medicare and Medicaid Services or the Joint Commission.
The two-tier sample included the nursing home’s direct clinical staff and patients with indwelling catheters. The maximum number of the home’s nurses and certified nursing assistants was involved (26). They were recruited to participate in a training program to ensure the appropriate use of 2% chlorhexidine gluconate washcloths. The number of patients who could be involved was limited to the potential maximum of ten because of the monetary costs of using 2% chlorhexidine gluconate washcloths. The total number of residents only amounted to four, however, since more participants were not available. It should be noted that a preliminary inquiry determined that many more residents could have been recruited, but because of changes in their state, location, or other factors, most of them became ineligible. The project had to demonstrate flexibility and adjust to the limitations of the site.
Inclusion/exclusion criteria
For the staff, the inclusion criterion consisted of them being a part of the site’s staff, and no exclusion criteria applied. The patients were voluntarily enrolled based on specific criteria, including age, medical condition, medication, and the presence of a urinary catheter. According to the initial plans, the eligible patients had to be admitted for more than eight weeks in the selected long-term care facility, aged 65 years and older (but younger than 89), not diagnosed with any urinary tract infection prior to the study, and not under any form of antibiotic treatment for any form of infection during the duration of the study. After it was established that no resident could test negative for leukocytes, the medical state criteria were modified, and the participants were enrolled despite having leukocytes in their urine.
Ethics and confidentiality
The risks of the project were not very high, especially for the staff. Still, the issues of voluntary participation, confidentiality, and protection of participants were reviewed before the project was implemented. The letters of approval from both the relevant institution (Appendix A) and site (Appendix B) were received. Consent was obtained from the participant or the participant’s immediate guardian. An extensive explanation of the purpose, procedures, advantages, disadvantages, and possible outcomes of the study was communicated to obtain the consent. All the participants received codes instead of names to facilitate the matching of the data and the protection of the residents and staff members. All the data were only used by the principal investigator, which limited their exposure; all the information is currently kept in a secure location under the control of the same person, and it will be destroyed in five years.
Budget and budget analysis
Table 1 presents the project’s budget. The costliest aspect was the intervention; the washcloths cost a little over $1,262, which may be considered a potential limitation of this intervention. The rest of the costs were associated with training activities, as well as staff meetings, and included learning materials, prizes for the members with the highest scores, and food.
Table 2. Budget.
Project implementation
The project focused on introducing the washcloths, teaching the staff of the site to use them, and applying them to a sample of residents for two weeks while monitoring their health and checking them for CAUTIs. A program was designed to educate and train nurses and nursing assistants assigned to bathing and cleaning the senior long-term care facility residents with 2% chlorhexidine gluconate washcloths. The program took 30 minutes, including a 20-minute lecture and a 10-minute hands-on demonstration. Instructional modules and printed materials were handed out for the nurses’ and nursing assistants’ reference.
Timeline of the project
Upon the IRB approval from South University, the following steps were undertaken.
- On August 6, 2019, a meeting was held with the nursing leaders, and it launched the program; a recruitment flyer was posted in several locations, including the first-floor main lobby (Appendix C), different activity locations, dining rooms, nursing stations, the conference room, and elevators of the site.
- Staff participants’ recruitment was completed with their informed consent.
- The staff training session took place (Appendix D); before and after the session, the staff participants filled out the questionnaire-based survey (Appendix E). The nursing staff was trained on the use of the tracking intervention tool. Soap, shampoo, lotion, and other skin barrier creams were prohibited from treatment areas to prevent skin reaction. A twelve-slide PowerPoint presentation, which detailed the proper step-by-step procedure relating to the correct use of the 2% chlorhexidine wipes, was used as a part of the nursing staff training. The 2% chlorhexidine wipes were ordered on August 6, 2019. As promised by the Sage company representative, the wipes were delivered on August 8, 2019.
- The director of the site assigned the task of bathing the residents with the wipes to the 7-3 shift. Another educational tool that was discussed with the nurses to check for signs and symptoms of CAUTI is “The CAUTI Assessment Profile (CAP)” (Appendix F). On August 8, 2019, training on the use of a checklist took place; the checklist was attached to a clipboard with an ink pen and placed at each resident participants’ bedside to be filled out and signed by staff participants. Three staff meetings took place.
- In collaboration and with approval from the site and medical director, potential residents were informed of the product, benefits, any risks, and the process for enrolling in the project. Some of the residents were not allowed to sign their own consent forms because their families did not want them to participate.
- Urine samples for the urinalysis were collected from potential resident participants as soon as all informed consents had been collected.
- The staff participants were involved in bathing and monitoring the residents selected for the study.
- At the end of the project, resident participants were retested for CAUTIs with the help of urinalysis.
- The efficacy of the intervention was assessed.
The timeline of the project is best presented in the form of Table 2. The latter shows that around two months were required to get the project approved, and after that, a month involved its implementation.
Table 3. The Timeline.
Methods, procedures, and instruments
Data collection
The data collection process was divided into two segments. The first part was related to the training program involving the members of the healthcare team. With the help of a survey, this information was collected before the training program and after it. The maximum number of nurses and certified nursing assistants were engaged in the program. The staff participants were then involved in bathing and monitoring the residents, who were selected for the study, during the two-week evaluation period and ensured that records of any infection would be noted.
Chlorhexidine’s effectiveness in the reduction of CAUTIs was examined using a pre-test post-test design as well; the residents’ state was measured prior to the institution of chlorhexidine baths and then compared to their condition after chlorhexidine bathing implementation. At the start of the evaluation period, each patient was tested for urinary tract infection with the help of a urinalysis. Only patients who would test negative were supposed to be eligible for the study, but because of the lack of such residents, this criterion was removed from the exclusion criteria. As a result, five patients who had leukocytes (two of them also had some nitrite) in their urine were recruited. In addition to bathing them as usual, the staff used 2% chlorhexidine gluconate washcloths.
If any participant had developed CAUTIs over the two weeks following their recruitment, the case would have been recorded to report CAUTI rates during the project. However, the patients did not develop CAUTIs. Four of the residents were tested once again with the help of urinalysis at the end of the two-week period. One of the initially recruited participants had to be disenrolled because they had to be moved to another unit; this event was not related to the project. For the purposes of the project, all the data were captured electronically and collected as datasheets for each resident and staff member before and after the implementation of the respective intervention (washcloths bathing and training).
Instruments
To measure the effectiveness of the training intervention, a knowledge checklist shown in Appendix E was utilized to gauge the level of understanding of the healthcare professionals. It was based on the information provided by the article by Jain et al. (2015) that is dedicated to nurses’ knowledge related to CAUTIs. It was also meant to represent the information from the training. As a result, it is relatively valid (that is, capable of measuring the CAUTI knowledge as reflected by the training session), but as a new tool, it did not receive reliability or validity testing.
Validity and reliability of the CAUTI Assessment Profile Screening Tool. While it is not an instrument proper, an assessment sheet (Appendix F), which details the proper step-by-step procedure for CAUTI detection, was used as educational material. It is evidence-based and has an established face validity based on specialists’ feedback; its reliability has been tested with kappa ranging between 0.29 and 0.79 (Blodgett, Gardner, Blodgett, Peterson, & Pietraszak, 2015). This tool can be used to demonstrate the type of information that was provided to the nurses during their training.
Outcome measures
In this evidence-based quality improvement project, the analysis included the participants’ demographic data, the professionals’ knowledge, and the patients’ urinalysis results. Descriptive statistics described the findings related to the demographic data and summarized the rest of the findings, including the results of the surveys and urinalysis. The CAUTI prevention knowledge scores were computed based on the number of correct answers before and after the training. Urinalysis was used to check the patients’ health and the presence or absence of CAUTI in the sample; specifically, leukocytes and nitrite were determined. These measures constitute a well-established approach to tracking CAUTIs (Shimoni, Hermush, Glick, & Froom, 2018).
Data analysis: statistical tests
The knowledge obtained by the participants was demonstrated by the changes in their pre- and post-training scores. The scores were determined by the self-developed instrument, which produced continuous data between 1 and 16. In order to test the pre- and post-training data for statistically significant differences, a t-test or its nonparametric alternative was required (Polit & Beck, 2017, p. 412). Due to the non-normal distribution, Wilcoxon signed ranks test was eventually employed. Two-tailed tests were used; statistically significant differences were checked to find out if the changes are positive (more correct answers) or not (more incorrect answers). A conclusion about the professionals’ pre- and post-intervention performance was made based on this information to show if the professionals involved in the project were likely to apply the intervention correctly.
The findings for the patients could be expressed through nominal data; basically, they tested either “positive” or “negative” for leukocytes or nitrite. However, urinalysis and culture analysis also produce continuous data (for bacteria, nitrite, and blood in urine), and this information was initially supposed to be collected before and after the patients were washed with the washcloths. Consequently, it was planned to use a test suitable for continuous data, including the paired t-test (Polit & Beck, 2017, p. 412). However, due to the lack of changes, the resident data was eventually just summarized. The lack of a statistically significant difference between pre- and post-test results would indicate that the condition of the participants did not worsen. This part of the analysis directly responded to the PICOT question, showing the effectiveness of the intervention at preventing CAUTI over the established period of time with the chosen population.
Minitab software was used to run the tests, and the collected data were inserted into a Minitab file. The data were checked and cleaned, and descriptive analyses were used to describe the results and determine if the t-test could be used. Then, the inferential tests were run with the commonly used significance level of 0.05 and confidence interval of 95 (Polit & Beck, 2017). Percentages and graphs were employed to represent the information in detail and visually. Microsoft Excel was used for creating the figures.
Summary
The presented project is a pre-test post-test quality improvement effort with urinalysis results (dipstick analysis) and CAUTI knowledge scores (special training-based tool) as the primary data collection methods. The project involved a training session for the staff of a long-term care unit that was aimed at the correct implementation of 2% chlorhexidine washcloths with the goal of reducing CAUTIs. The results of this project will be reported in the next chapter.
Findings
Results/Outcomes
Descriptive results
Table 1 summarizes the demographics of the sample, as well as the averages of their scores.
Table 4. Demographics Summary (Staff).
As can be seen from Figure 1, 26 people were recruited; 100% of them were female. Exactly 50% of the sample consisted of nurses; the rest were nursing assistants (see Figure 1).

Most participants were older than 30 (see Figure 2). Only six people (approximately 23% of the sample) were younger; nine of the participants (33%) were aged between 31 and 40, and six more people (roughly 22%) reported being between 41 and 50 years old. Also, five people were older than 51 but younger than 60, and one participant was older than that.
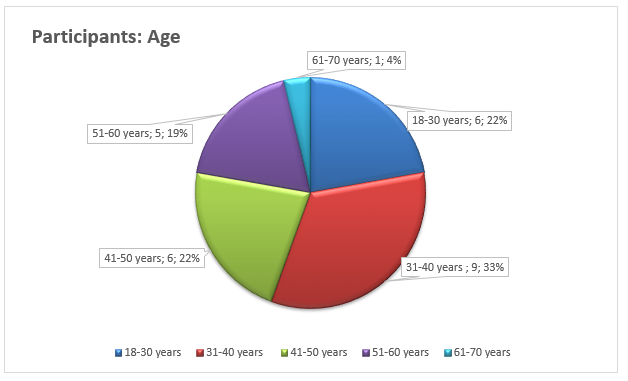
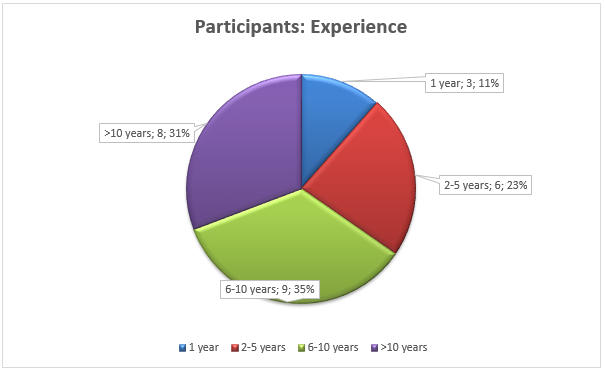
Figure 3 demonstrates that most participants had six years of experience or more; only three of them (a little over 11%) reported having the working experience of one year, and six of them (around 23%) had been working for two-to-five years. Nine people (roughly 35%) had worked for more than six years but less than ten years, and the rest of the participants (31%) had the experience of over ten years of work. To summarize, the sample included female nurses and nursing assistants, and the majority of them were older than 30 and rather experienced.
The patient CAUTI status was determined with the help of dipstick urinalysis. As can be seen from Table 3, which summarizes the results and specifies the dates of data collection, tests returned positive for leukocytes for 100% of the patients; 40% of them also had nitrite in their urine. However, none of them presented with any CAUTI symptoms, which is why it was determined that they could be enrolled in the project. One of the patients (Star 9093) had to be transferred to another site for reasons that were not related to the project. The rest of the patients showed no changes in their analyses (or symptoms) during the post-test data collection. Since no differences between the measurements exist, no statistical analysis beyond descriptive statistics (percentages) has been applied to these data.
Table 5. Pre and Post Urinalysis Results for Patients.
Statistical results. The goal of this analysis was to determine if any relationship between the independent (intervention) and dependent (survey score) variables can be found. Minitab conducted tests to check for normality, which showed that one of the datasets was not normally distributed; the histogram supported the idea (see Figures 4 and 5). In other words, the t-test could not be applied to these data; instead, as indicated by Polit and Beck (2017), it was necessary to use the Wilcoxon signed ranks test.
Checking the differences between the datasets is required to conduct the Wilcoxon signed ranks test in Minitab (Looney & Hagan, 2015). For this sample, the mean, median, and mode of the differences in the scores equal 2, and their box graph shows that this dataset is relatively symmetric (see Figure 6), which qualifies it for the Wilcoxon signed ranks test.
Table 2 details the results of the Wilcoxon signed ranks test run by Minitab. The significance is below the initially established level of 0.05 (p=0.004), which means that a statistically significant difference has been proven to exist between the two samples (Polit & Beck, 2017). Consequently, it can be assumed that the tested intervention had an impact on the participants’ scores, which measure the team’s ability to prevent CAUTI and apply the 2% chlorhexidine washcloths. Therefore, the statistical analysis indicates that after their training, the participants became better qualified to take care of patients and utilize the washcloths.
Table 6. Wilcoxon Signed Ranks Test for the CAUTI Nurse Survey Results.
Discussion/Conclusions
This section will present a discussion of the findings of the CAUTI prevention project. The analysis of the nursing staff’s data suggests that the nurses and nursing assistants were all women; the majority of them were older than 30 and relatively experienced. Furthermore, their scores showed a statistically significant improvement as a result of the CAUTI prevention training that they received. The purpose of this part of the project was to ensure that the nursing staff could employ the project’s intervention (washcloths) correctly. The analysis results prove that the training was effective, the implication being that the staff should have been able to apply the washcloths.
In addition, the training was helpful as a quality improvement effort since it resulted in some meaningful improvement of the participants’ knowledge; the implication is that it can be recommended for future efforts. However, the training was tested with a limited sample (26 people) in one institution; also, all of the participants were female, although a level of diversity in age and experience could be observed. Therefore, this implication should be considered with all the related limitations.
The patient data demonstrate no changes in the patients’ health before and after the application of chlorhexidine washcloths. Therefore, the findings suggest that the patients did not develop new CAUTIs during the project, which is in line with the very strong evidence that indicates the effectiveness of the washcloths bathing in CAUTI prevention (Huang et al., 2016). However, the intervention was applied to only a few patients who had already tested positive for leukocytes prior to the intervention’s implementation, which is a limitation.
To summarize, the project presents relatively strong evidence to the effectiveness of the project’s training, but its evidence to the preventative qualities of 2% chlorhexidine gluconate washcloths is less notable. The sampling limitations are the main ones to consider when discussing the implications of the project. The training can be recommended in other similar cases, and the lack of CAUTI development in the sample can be considered a contribution to the pool of the data indicating the effectiveness of washcloths in preventing CAUTIs.
Project Strengths and Limitations
Strengths
For this project, its topic can be considered a strength since, as shown by the literature review, the specific combination of its setting and intervention may not have been very extensively researched. In addition, the methods that were employed were based on evidence, including the intervention, training tool (see Appendix F), and urinalysis. Finally, the chosen model is a common one that has been used to structure many nursing and healthcare projects.
Limitations
It should be emphasized that the project’s sample may have caused significant limitations. Regarding the staff, 26 members (nurses and nursing assistants) were available. While the differences in their knowledge prior to and after the training were statistically significant, it is still a relatively small sample that comes from one specific site. Residents were even less numerous; given the project’s extensive eligibility criteria, only five people were recruited. Moreover, one of them was transferred before the washcloth implementation; the project only managed to collect the pre-test urinalysis results for that resident. Consequently, four residents constituted the final sample of the project, which implies that the findings should not be treated as very generalizable.
Moreover, all the urine samples that were collected throughout the project had leukocytes in them, and two of them also had nitrite. Initially, the project was supposed to involve the residents who tested negative, but the site did not have such residents. As a result, the residents who did not exhibit CAUTI symptoms were viewed as eligible, and the project tracked changes in their health. Since none were recorded, the intervention appears to have prevented the development of new CAUTIs. Still, this feature of the sample needs to be considered. The issue of the CAUTI knowledge tool, which has not been fully tested for validity or reliability should be mentioned as well. Finally, the project did not take very long; it cannot yield any information about the long-term application of the washcloths. In summary, the ability of this project to offer generalizable results is limited by several important features.
Conclusions, Recommendations, and Implications for Practice
Project Summary
This project, which was also a quality improvement effort, was devoted to CAUTIs, as well as their prevention and rate reduction. The general aim was to decrease the likelihood of developing CAUTIs among the residents of a long-term care facility, as well as testing an intervention that is evidenced to achieve such an outcome (2% chlorhexidine washcloths) (Huang et al., 2016). Long-term care residents, especially if they are older adults, are a vulnerable population when CAUTIs are concerned (Jump et al., 2018), which justified the interest in the topic. The project employed the staff and residents of the facility.
The former group of participants was trained to ensure the correct usage of the intervention; the latter group was subjected to regular washcloth bathing. The effectiveness of both the training and intervention were measured before and after their application with statistical analysis applied as appropriate. In this section, the results and conclusions will be summarized, and the possibility of future projects will be examined.
A questionnaire was used to test the staff’s CAUTI knowledge. It allowed determining the impact of the training on the participants’ ability to prevent CAUTI, and the application of the Wilcoxon signed ranks test indicated that the training was indeed effective (p=0.004). The residents’ urinalysis results were employed to assess their health. Their state did not change by the end of the procedures, which implied that the washcloths might have been successful in lowering the likelihood of CAUTI development. Thus, the project managed to achieve the objective of ensuring a decreased probability of CAUTIs, and it also successfully improved the staff’s knowledge in an attempt to enable the correct usage of the tested intervention. The findings need to be considered along with the restrictions of the project, including its small duration and samples. However, future research may assist in rectifying the issue, and the current project has achieved its objectives while also improving the quality of care delivered by the site’s nurses and nursing assistants.
Implications for Nursing Practice and to the DNP Essentials
Implications for nursing practice
The project identifies the problem of CAUTI knowledge among nurses; it suggests that the site’s nurses might require more training. The training program was shown to be effective with a small sample; it might be applicable in similar circumstances. The evidence for 2% chlorhexidine washcloths is not enough to support their implementation in nursing homes.
Connection to the DNP essentials
From the perspective of the implications for the researcher, the project consisted of researching and implementing an evidence-based practice while using leadership and problem-solving skills in an interprofessional team. These factors correspond to the essentials of the American Association of Colleges of Nursing (2006).
Implications for health care delivery
The project is directly connected to healthcare delivery problems because it inadvertently discovered an issue that might prevent the nursing staff from effectively applying the studied intervention, as well as other CAUTI-related measures. The project demonstrates the importance of ongoing training for nurses of all ages and levels of experience, which may be especially significant for the project’s site due to its high prevalence of CAUTIs.
Future research
Future projects should be able to rectify the presented concerns and expand the knowledge on CAUTI reduction and prevention. First, a larger sample, as well as samples from several sites, could be a good opportunity to investigate the application of the washcloths in long-term care. This suggestion is especially true for the resident’s data, which were not sufficiently robust for conclusive statements in this project. In addition, it would be very helpful to attempt to introduce a sample of residents who test negative for leukocytes and nitrite. Finally, extending the timeframe of the application of washcloths would yield the long-term data that this project cannot offer.
It should be noted that this project did not view the training of the nurses and nursing assistants as its primary aspect, but this activity was still important for the correct use of the intervention. In addition, the training allowed the project to advance the participants’ CAUTI knowledge, which is a significant outcome for a quality improvement effort. Therefore, a large or more diverse sample of staff members would also be useful in further investigating the efficacy of the training. A future project might focus exclusively on this aspect of CAUTI prevention as well. In general, additional research can produce evidence that will complement this project’s findings and avoid its limitations.
Dissemination methods
This project will be presented to the researcher’s peers, and a manuscript for the American Journal of Nursing has been developed. Hopefully, it can attract attention to the issue of CAUTI prevention in long-term care, which is not very well reflected in recent literature.
Summary
Based on the findings, the site might require additional CAUTI training for its nursing staff, although the project has already contributed to resolving this concern. Furthermore, the project did produce some information that is pertinent to CAUTI prevention with 2% chlorhexidine washcloths, but it is not sufficient for definite and conclusive statements. Future research should use the findings and avoid the pitfalls of this project.
References
AACN Practice Alert. (2016). Prevention of catheter-associated urinary tract infections in adults. Critical Care Nurse Journal, 36(4), 9-11. Web.
Afonso, E., Blot, K., & Blot, S. (2016). Prevention of hospital-acquired bloodstream infections through chlorhexidine gluconate-impregnated washcloth bathing in intensive care units: A systematic review and meta-analysis of randomized crossed trials. Euro Surveillance, 21(46). Web.
American Association of Colleges of Nursing. (2006). The essentials of doctoral education for advanced nursing practice. Web.
Amirov, C., & Candon, H. (2015). Chlorhexidine gluconate-impregnated washcloths reduce MRSA incidence in an endemic chronic care hospital: A randomized clinical trial. American Journal of Infection Control, 43(6), S5-S6. Web.
Blodgett, T., Gardner, S., Blodgett, N., Peterson, L., & Pietraszak, M. (2015). A tool to assess the signs and symptoms of catheter-associated urinary tract infection. Clinical Nursing Research, 24(4), 341-356. Web.
Cao, Y., Gong, Z., Shan, J., & Gao, Y. (2018). Comparison of the preventive effect of urethral cleaning versus disinfection for catheter-associated urinary tract infections in adults: A network meta-analysis. International Journal of Infectious Diseases, 76, 102-108. Web.
Carter, N., Reitmeier, L., & Goodloe, L. (2014). An evidence-based approach to the prevention of catheter-associated urinary tract infection. Urologic Nursing, 34(5), 238-245. Web.
Centers for Disease Control and Prevention. (2013). Urinary Tract Infection (UTI) event for long-term care facilities. Web.
Centers for Disease Control and Prevention. (2017a). Data summary of HAIs in the US: Assessing progress 2006-2016. Web.
Centers for Disease Control and Prevention. (2017b). National and state healthcare-associated infections progress report. Web.
Cummings, S., Bridgman, T., & Brown, K. (2016). Unfreezing change as three steps: Rethinking Kurt Lewin’s legacy for change management. Human Relations, 69(1), 33-60. Web.
Delesie, L., Blot, S., Vanacker, T., & Vandijck, D. (2011). Implementation of chlorhexidine gluconate in the prevention of line-related infection. American Journal of Infection Control, 39(4), 346-347. Web.
Durant, D. J. (2017). Nurse-driven protocols and the prevention of catheter-associated urinary tract infections: A systematic review. American Journal of Infection Control, 45(12), 1331–1341. Web.
Gefter, J., Zaks, B., Kirmayer, D., Lavy, E., Steinberg, D., & Friedman, M. (2018). Chlorhexidine sustained-release varnishes for catheter coating – dissolution kinetics and antibiofilm properties. European Journal of Pharmaceutical Sciences, 112, 1-7. Web.
Huang, H., Chen, B., Wang, H., & He, M. (2016). The efficacy of daily chlorhexidine bathing for preventing healthcare-associated infections in adult intensive care units. The Korean Journal of Internal Medicine, 31(6), 1159-1170. Web.
Jain, M., Thakur, A., Dogra, V., Mishra, B., & Loomba, P. (2015). Knowledge and attitude of doctors and nurses regarding indication for catheterization and prevention of catheter-associated urinary tract infection in a tertiary care hospital. Indian Journal of Critical Care Medicine, 19(2), 76-81. Web.
Jump, R., Crnich, C., Mody, L., Bradley, S., Nicolle, L., & Yoshikawa, T. (2018). Infectious diseases in older adults of long-term care facilities: Update on approach to diagnosis and management. Journal of the American Geriatrics Society, 66(4), 789-803. Web.
Lewin, K. (1947). Group decision and social change. Readings in Social Psychology, 3(1), 197-211.
Looney, W. S., & Hagan, L. J. (2015). Analysis of biomarker data: A practical guide. Hoboken, NJ: John Wiley & Sons.
McCoy, C., Paredes, M., Allen, S., Blackley, J., Nielsen, C., Paluzzi, A., … Radovich, P. (2017). Catheter–associated urinary tract infections: Implementing a protocol to decrease incidence in oncology populations. Clinical Journal of Oncology Nursing, 21(4), 460–465. Web.
Mitchell, B. G., Fasugba, O., Cheng, A. C., Gregory, V., Koerner, J., Collignon, P.,… Graves, N. (2019). Chlorhexidine versus saline in reducing the risk of catheter associated urinary tract infection: A cost-effectiveness analysis. International Journal of Nursing Studies, 97, 1-6. Web.
Nicolle, L. E. (2014). Catheter associated urinary tract infections. Antimicrobial Resistance and Infection Control, 3(23), 1-8. Web.
Noto, M., & Wheeler, A. (2015). Understanding chlorhexidine decolonization strategies. Intensive Care Medicine, 41(7), 1351-1354. Web.
Noto, M., Domenico, H., Byrne, D., Talbot, T., Rice, T., Bernard, G., & Wheeler, A. (2015). Chlorhexidine bathing and health care–associated infections. JAMA, 313(4), 369-378. Web.
Peter, S., Devi, E. S., & Nayak, S. G. (2018). Effectiveness of clinical practice guidelines on prevention of catheter-associated urinary tract infections in selected hospitals. Journal of Krishna Institute of Medical Sciences, 7(1), 55–66. Web.
Polit, D. F., & Beck, C. T. (2017). Nursing research: Generating and assessing evidence for nursing practice (10th ed.). Philadelphia, PA: Lippincott, Williams & Wilkins.
Popovich, K., Lyles, R., Hayes, R., Hota, B., Trick, W., Weinstein, R., & Hayden, M. (2012). Relationship between chlorhexidine gluconate skin concentration and microbial density on the skin of critically ill patients bathed daily with chlorhexidine gluconate. Infection Control & Hospital Epidemiology, 33(9), 889-896. Web.
Rhee, Y., Palmer, L. J., Okamoto, K., Gemunden, S., Hammouda, K., Kemble, S. K.,… Yokoe, D. S. (2018). Differential effects of chlorhexidine skin cleansing methods on residual chlorhexidine skin concentrations and bacterial recovery. Infection Control & Hospital Epidemiology, 39(4), 405-411. Web.
Schmudde, Y., Olson-Sitki, K., Bond, J., & Chamberlain, J. (2019). Navel to knees with chlorhexidine gluconate. Dimensions of Critical Care Nursing, 38(5), 236-240. Web.
Scott, G. (2016). Nurse-led practice is a model for change. Nursing Standard, 30(26), 3. Web.
Shimoni, Z., Hermush, V., Glick, J., & Froom, P. (2018). No need for a urine culture in elderly hospitalized patients with a negative dipstick test result. European Journal of Clinical Microbiology & Infectious Diseases, 37(8), 1459-1464. Web.
Shippey, S., & Malan, T. (2004). Desquamating vaginal mucosa from chlorhexidine gluconate. Obstetrics & Gynecology, 103(5 Pt 2), 1048-1050. Web.
Sinha, A., Sazawal, S., Pradhan, A., Ramji, S., & Opiyo, N. (2015). Chlorhexidine skin or cord care for prevention of mortality and infections in neonates. Cochrane Database of Systematic Reviews, 5(3), 1-59. Web.
Strouse, A. (2015). Appraising the literature on bathing practices and catheter-associated urinary tract infection prevention. Urologic Nursing, 35(1), 11-17.
Swan, J. T., Ashton, C. M., Bui, L. N., Pham, V. P., Shirkey, B. A., Blackshear, J. E.,… Butler, M. O. (2016). Effect of chlorhexidine bathing every other day on prevention of hospital-acquired infections in the surgical ICU. Critical Care Medicine, 44(10), 1822-1832. Web.
Trautner, B. W., Greene, M. T., Krein, S. L., Wald, H. L., Saint, S., Rolle, A. J.,… Mody, L. (2017). Infection prevention and antimicrobial stewardship knowledge for selected infections among nursing home personnel. Infection Control & Hospital Epidemiology, 38(1), 83-88. Web.
Wang, Z., Zheng, J., Zhao, Y., Xiang, Y., Chen, X., Zhao, F., & Jin, Y. (2017). Preoperative bathing with chlorhexidine reduces the incidence of surgical site infections after total knee arthroplasty. Medicine, 96(47), e8321. Web.
Appendix
Education Flyer

Pre- and Post-Education Survey
Demographic Characteristics (circle)
Response Key (Circle Response to each question/statement below)
Long-term use of Urinary catheters, such as Foley or suprapubic is appropriate for the following conditions:
- Urinary retention that cannot be managed by intermittent catheterization 1 2 3 4 5 6
- Large pressure ulcers 1 2 3 4 5 6
- Terminal illness that makes bed clothing changes uncomfortable for the resident 1 2 3 4 5 6
The following questions concern personal hygiene when caring for residents with indwelling urinary catheters:
- I cleanse my hands with soap and water or alcohol-based hand rub before urinary catheter manipulation 1 2 3 4 5 6
- It is not necessary to cleanse hands after casual contact, such as taking pulse or adjusting their position with residents with urinary catheter 1 2 3 4 5 6
- If my hands are not soiled, hand hygiene with alcohol-based hand rub is adequate after manipulation of catheter site 1 2 3 4 5 6
- It is not necessary to wash my hands with soap and water after removing gloves 1 2 3 4 5 6
- Gloves must be worn when caring for residents with indwelling urinary catheter 1 2 3 4 5 6
The following measures should be taken for care of residents with indwelling urinary catheter:
- Area around urinary catheter cleansed at least once a day 1 2 3 4 5 6
- Catheter should be changed once a month 1 2 3 4 5 6
- Catheter and its bag can be temporarily disconnected 1 2 3 4 5 6
- Catheter should be irrigated once per week 1 2 3 4 5 6
- Catheter can be inserted for nursing staff convenience 1 2 3 4 5 6
- CAUTI is not a very serious illness 1 2 3 4 5 6
- Education regarding basic catheter care helps prevent CAUTI 1 2 3 4 5 6
- Catheter care is done in a one-way manner from the meatus to the connection to the drainage bag 1 2 3 4 5 6
- Catheter should be removed whenever it is convenient for hospital care professionals 1 2 3 4 5 6
Tracking Intervention Skin Monitoring: The CAUTI Assessment Profile (CAP)
A Tool to Assess the Signs and Symptoms of Catheter-Associated Urinary Tract Infection
Subject ID:_________________________ Rater Initials:_____________________
Date of Visit:_______________________ Unit:_____________________________
Delirium
If features 1 and 2 and either 3 or 4 are present, delirium is “Present” (Inouye, Van Dyck, Alessi, Balkin, Siegal, & Horwitz, 1990)