Introduction
Quality is rapidly becoming a global issue as well as a concern to both the suppliers of services and the consumers of those services. In healthcare, quality is reaching a new dimension in that, it is being demanded and expected thus providers are judged by it. Health care quality is becoming a required attribute to providing care whether in United States, Europe, Asia, or any other part of the world (Al-Assaf 1998). Several reasons could be mentioned as to why quality is needed and why we ask for quality. Some of these reasons are :Increased demands for effective and appropriate care, need for standardization and variance control, necessity for cost saving measures, benchmarking, accreditation, report cards on provider performance, requirement to define and meet patient needs and expectations, need for improvements in care and services, desire for recognition and the strive for excellence, competition, and ethical considerations (Al-Assaf 1998).Introducing the real meaning of the term Quality might be slightly odd to some readers who are not exposed to what quality means. It has been identified by many of its gurus whether the Americans or the Japanese. It was defined by Joseph Juran as “fitness for use” (TQM.MN7322/D© University of Leicester 2007, p. 15). The other view of Philip Crosby advocated the ‘conformance to requirement’ which has been referred to as ‘Zero defects’. In other words Total Quality Management is a process which embraces the conscious striving for zero defects in all aspects of an organisation’s activities (TQM.MN7322/D© University of Leicester 2007 p. 110). In health care, another definition of quality may apply. Quality is doing the right thing the first time and doing better the next (Al-Assaf 1998).
Nationally, Saudi Arabia has witnessed a massive improvement in socio-economic development in the past 30 years, with profound progress in health, education, housing and the environment. Research and quality assurance are recognized as being crucial for the development of the health system.
According to (Patrice1998) it is justifiable that the successful quality management process requires a commitment by the board to visibly support the quality mission of the organization. This transformation starts with board education. Board members should be introduced to the principles, tools, and techniques of continuous quality improvement. Activating the role of quality in hospitals’ system is the real measurement tool to be evaluated in hospitals’ process and procedures. The measurement bodies which are considered as great awards are CBAHI (Central Board for Accreditation of Healthcare Institutions) & JCI (Joint Commission International). This accreditation and certification is the proven process your organization needs to help ensure a safe environment for your patients, staff and visitors. This voluntary process shows your organization’s commitment to continuously improving patient safety. One of these measures and processes to be monitored is Capacity management in each hospital. The definition of this process stated as” Adjustment of the capacity of a resource (equipment, machine, or system) to meet a planned demand or load. In general, manufacturing capacity may be adjusted by working overtime or redeploying the manpower”(Business Directory, 2011, p.1). This policy provides healthcare staff with guidance in relation to bed capacity management setting out patients flow standards, discharge actions on the day and clear explanations of roles and responsibilities for wards and departments as well as individuals at ward and departmental level and trust wide roles and responsibilities. This policy will outline the principles and processes required for effective bed capacity management (Orion, 2002, p. 1)
A huge quantity of statistics, facts, figures and numbers are registered on daily basis by Information technology department. These clinical processes give data that is valuable and useful for smooth functioning, decision making and improving processes. However, this data could be used for setting up the priority of any organisation if the leader of study is intensive in his teamwork. Data can become useful only if relevant information can be extracted out of it which is not ordinarily seen or understood (Witten & Frank, 2005) and converted to usable information for the organisation. This is a difficult task that is made easier through Data Mining. This has become necessary as a business needs this data to be translated into understandable information, and to uncover the patterns of transactions and processes. Such information is helpful in making informed business decisions based on facts.
The Need and Significance of the Study
Capacity resources such as facilities, equipment, and workforce can influence the selection and timing of services offering, the quality of service, the cost of service, as well as the satisfaction of customers, employees and payers. Recent healthcare research in other countries has focused on the development and adoption of more effective capacity resource management decisions (Li and Benton, 1996; Smith-Daniels et al., 1988; Siferd et al., 1994). These efforts have been made by the above authors published in European Journal of operational research.
Saudi Arabia has no research to measure the impact of Decision making strategy on utilizing priority setting and program data. Healthcare organizations of Saudi Arabia have little understanding of that matter. Public hospitals organizations in Saudi Arabia are utilizing Data for conducting new project if there is lack of facilitates. It was a reaction to what is usually missing. No one does research to check the role of consumer needs in determining the services delivery, quality and organization’s outcome. This dissertation is aimed at answering the questions of unsolved issues on bed capacity situations in Hera General Hospital to be used by other organizations.
Organizations dealing with capacity issues have several options, including: Increasing capacity within current licensed space, building more beds, adding functional capacity through improving patient throughput and smoothing demand through variability isolation. However, these options need clear study based on data and measurements.
Aims & Objectives
Patients’ needs for available bed is the real motivation for whoever has a conscious brain to take the issue for studying and finding solutions to be implemented for creating a better healthcare atmosphere.
The objective of this dissertation is expected to produce the following results: More effective capacity management, improved safety of care delivery, and develop a higher level of patient satisfaction and quality service. The following benefits could explain the effective role of capacity management in details:
- Quickly find available beds matching the specific needs of the patient for appropriate level of care placement.
- Reduced ED wait times for a bed.
- Pending discharges to provide dietary, housekeeping, pharmacy among other services with information helpful to planning staff needs as well as control costs on meals and medications that may be wasted.
- Increased patient, physician and employee satisfaction as result of efficient operational processes and utilization of resources for expediting placement and delivery of care.
- Reporting tools provide information on throughput initiative and staff performance for on-going performance improvement.
- Manages transport workflow, improving flow of patient movement throughout the facility.
- Sharing of key patient care and resource utilization information for efficient and effective care delivery as well as seamless communication among the bed management and care coordination teams.
The Research Questions
The main focus of this research will be to define the existing bed capacity situation of Hera General Hospital. Furthermore, this research aims to investigate the following questions:
- What are the main strategies of capacity management in Hera General Hospital?
- What are the key indicators of hospital capacity management that influence decisions in Hera General Hospital?
- How the hospital’s quality performance from program data, have an influence on such decisions?
- What are the possibilities for forecasting future capacity management for sudden crises, particularly during the Umrah and Hajj season (crowded seasons)?
Research Methodology
The main aim of the research will be to highlight different types of strategies that may solve the issue of hospital capacity in terms of forming the priorities through data utilization. To achieve this, the research project will be based on a combination of methods. In our fieldwork, a case study method will be adopted. Sample case studies are carried out to identify the nature of the work that is necessary to be done to gather the accurate set of information. This can be in single or in multiple study cases or even for the sample group (Yin, 1984). In addition, interviews will be conducted with the concerned members of the Bed Utilization Committee, as well as the Hospital Director, along with physicians and nurses. The reason for selecting interviewing as the primary research method is the adaptability it offers. This is something that cannot be achieved through surveys, especially if the members are uncooperative in the way they answer, and involve themselves in the problems as well as solutions. In another study on “Hospital capacity, Patient Flow, and Emergency Department Use in New Jersey” by (Derek Delia 2007) was conducted using interviews with key informants from the hospital in New Jersey. Informants included ED directors, nurse managers, and patient flow managers.
Observations guide will be designed to obtain the findings from the persons involved, and interpret the difficulties they mention into a clear format to contribute in solving the issue. The interviews will be structured with the various questions based on a number of areas developed via the literature review, in order to ensure that all of the significant issues are covered. These questions will be designed to uncover facts rather than opinions, which can often be unreliable, changeable and not always subjective.
Program Data from ITD (Information Technology Department) will be used to obtain the data concerning hospital occupancy statistics, and this is calculated according to admission-and-discharge processes, as well as length of stay as used by (Seug- Chul Kim, Ira Horowitz, Karl K. Young, Thomas A.Buckley, 1999, 36-46) in their study analysis of capacity management in the intensive care unit in a hospital. The data will be gathered using inpatients: number of admissions and discharges per month for the years 2004-2008, including bed occupancy rate in the In-patients departments and the Emergency Department. It is essential that figures are collected accurately to determine various forms of statistics, as well as conducting further fieldwork to collect primary data as well. Coordination with the hospital director, as well as committee members, was granted by the chairman of the committee. (See Appendix A and B)
Secondary data will be collected from books, journals and articles from libraries. Several methods such as the ratio method, discrete simulation, stochastic simulation and queuing models, have been suggested in the literature to solve the problem of bed planning (Ali Kokangul 2008).
Contributions of the Research
This research is expected to contribute to theory by incorporating concepts across disciplines for a holistic view of the required essentials for Bed Capacity Management in KSA hospitals. It also intends to state the main strategies used in Hera’a General Hospital to activate the role of Medical Team to have good utilization by implementing the policies and procedures of bed capacity program. Moreover, it is for guiding the decision makers by using the key indicators of hospital capacity management and polishes their decisions with quality concept to reassure their actions. It is also aimed at answering in brief those who wonder what is role of Mecca Hospitals during overcrowded seasons particularly in Umrah and Hajj season.
Limitations
It must be pointed out that in such a study conducted at the student level there are several constraints. Time, resources and capabilities are all limited, and due to these factors the research will be more indicative than assertive. However, since the study is considered as first study in Saudi Arabia, it is expected that it can bring forth some new knowledge that can become the cornerstone of a larger research effort for the concerned readers. In the Middle East I found no research related to deal with and that gave me a tough time to look for books and researches in UK and USA which had earlier discussed such issues.
Outline of this Dissertation
The remainder of the Thesis is organized as follows:
Chapter 1 presents a summary of implementing quality in healthcare organization. The definition of the quality was mentioned to give a clear view for the readers about it. Definition of capacity management is also stated to generalize the first impression of my dissertation. The objective of this study is to answer the questions of unsolved bed capacity situations in HGH to be used by other organization. The objective and aims were listed to highlight the significant of patients’ care in hospitals which deals with bed capacity management as one of its priority. Research methodologies include a case study of HGH in this dissertation and interviewing the related staff for the required issues. Observations guide was a tool used for having more details of the suggested facts. The contributions of the research are mainly to have the best utilization of priority setting and program data in effecting the program of bed capacity management.
Chapter 2 presents a theoretical overview of capacity management including the strategies, the key indicators of hospital capacity management that influence decisions makers to take actions and the impact of the hospital’s quality performance. Furthermore, it makes it possible to forecast future capacity management for sudden crises, particularly during the Umrah and Hajj season.
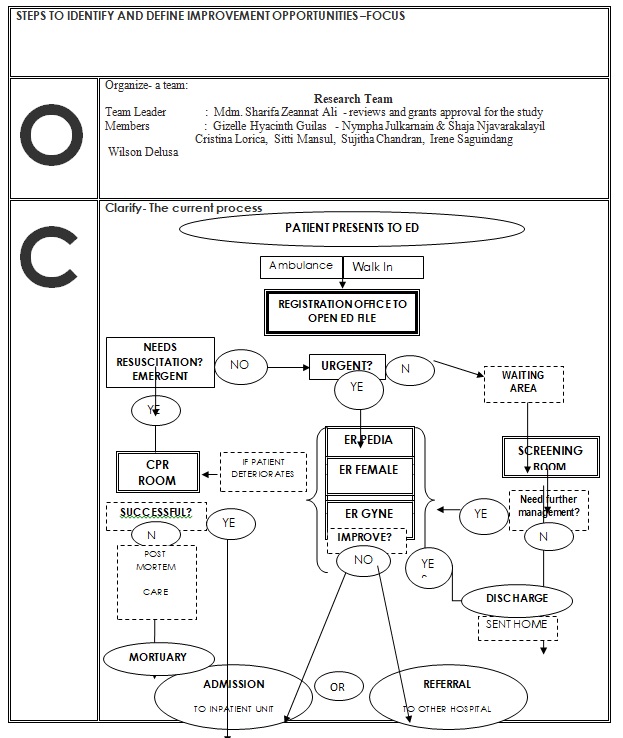
Chapter 3 explains the Research Methodology definition and the reasons for selecting Case study and Interview particularly for this dissertation. It gives a background of HGH quality experience since it established the quality department. It is a spotlight of how utilizing program data and priority setting criteria could give the guide for the organization to select, discuss and solve the problems. The measurement of ED overcrowding and patients flow are clearly discussed. HGH methodology in conducting the study is FOCUS-PDCA. It is the familiar quality tool in hospital.
Chapter 4 summarizes and addresses the findings of the bed capacity in HGH compared to NJ and follows them up with an in-depth analysis. It continues with a presentation of the experimental work and explains the methods used to evaluate and enhance the results.
Chapter 5 concludes the dissertation with an advice and recommendations for HGH and other KSA hospitals which face the same problem.
Literature Review
Introduction
The definition given From Wikipedia, the free encyclopaedia for what a literature review means is that “it is a body of text that aims to review the critical points of current knowledge including substantive findings as well as theoretical and methodological contributions to a particular topic” (Wikipedia). Literature reviews are secondary sources, and as such, do not report any new or original experimental work.
This study is a pilot study based in the Kingdom of Saudi Arabia which will address capacity management. There is much expectation that gathering baseline data from Hera General Hospital will ultimately be used as a reference for other hospitals. In response to this problem about increasing the numbers of patients in Emergency Department with no solutions for utilization of hospital bed capacity for In-patients departments especially during hospital surge capacity. This trend has implications beyond the ED as it signals problems or dissatisfaction with the performance and accessibility of local primary care delivery systems (Billings, Parikh, and Mijanovich, 2000-a).
Capacity management Strategies affect the direction of decisions makers
Clearly, US hospitals in the 1990s became very different from hospitals in the 1970s and 1980s due to progress. Changes in equipment, data technology, staff capabilities, patient expectation, and reimbursement methodologies have all contributed towards these differences. “In response to the current health service environment, the linkage between capacity management and performance has been underscored. Results from both empirical and theoretical research suggest that, “successful health service organizations tend to have superior capability for managing their capacity resources” (Flood and Scott, 1987; Smith-Daniels et al., 1988). HGH has utilized the monthly statistics report by Information Technology Department (ITD) in order to carry out further study and analysis. The formation of the Bed Utilization Program and appointment of Discharge Planning Officer were the result of decisions based on the program Data.
Ali Kokangul (2008) stated in his research that, “A combination of deterministic and stochastic approaches to optimize bed capacity in hospital unit, and that the ratio-based method can be applied to determine the size of the required capacity”. HGH used FOCUS-PDCA method, which was described as the average waiting time to tackle this problem.
With reference to Jee-In Hwag (2005) who described the level of emergency department (ED) volumes according to the hospital characteristics in order to identify the relationship between hospital capacity and ED volumes in Korea. These results help to show that ED volumes are indeed related to nursing, staffing, inpatients per bed, and the population in the area where hospitals are located. In relation to Hera Hospital, again the ED volume provided clear evidence that different issues which were studied by the Executive committee with the concerned members required the resultant expansion of ED bed capacity with complete facilities designed in a new building.
Most of the theoretical studies mentioned above have addressed capacity issues and their effects on performance, considering quality and patient safety through tracking metrics that drive patient’s flow; in order to produce accurate data on the patient discharge process, which increases available capacity.
Impact of the key indicators of hospital capacity management on decisions
Recent healthcare research in other countries has focused on the development and adoption of more effective capacity resource management decisions. The key indicators of hospital capacity resource management decisions are: outpatient’s services, healthcare network, workforce competence, and information technology (Li and Benton, 1996; Smith-Daniels et al., 1988; Siferd et al., 1994). These were one of the managerial insights emerged in the mentioned research. The focus of Hera General Hospital on capacity management resource processes, such as: facilities; equipment; the workforce, which clearly influences the selection and the timing of the service offered; the quality of service; the cost of service, and the satisfaction of customers as well as employees, which are important in anticipating the problem of capacity. The key indicators of HGH are hospital information technology, Department statistics and workforce competence and these are considered as the guidance to take actions by the decisions makers. These indicators are affected by some factors which include;
Hospital factors
Hospitals vary greatly in demographic factors (hospital size, location, and teaching involvement) and service mix characteristics are often used to categorize hospitals and used as a scheme to compare hospitals’ capacity management decisions (Comparative Performance of US hospitals, 1993: The Guide). The hospitals’ size factor is determined by the numbers of beds (Hancock et al., 1976 Nath and Sudharshan, 1994). Therefore, if the larger hospitals fail to manage their facility utilization appropriately; this will affect the quality performance compared to their competitors. The Table.1 below shows the numbers of beds in HGH.
Hospital Location is another factor that is likely to have an effect on capacity decisions. The location of a hospital in rural area as opposed to an urban area influences its facility management choice. For example, increased distance has a negative effect on hospital facility utilization (Abernathy and Hershy, 1972). HGH is located in North of Mecca city and it covers several primary healthcare centres. According to (Henry, 1994; Hudson, 1995) who stated that Hospitals in rural areas have been reinventing their capacity management strategies to match their competition, especially in the area of workforce management because demand for different type of labour skill is low and staff members have to be more versatile. This is in relation to HGH which suffered much from having full numbers of staff required for Emergency department in particular either doctors or nurses. Moreover, it has been noticed that some of the ED staff are not fully trained for dealing with the procedures there. That encourages the higher administration to assign two consultants to work on educational activities and update them with the related knowledge.
Hospital teaching involvement is another factor that may affect hospital capacity decisions (Flood and Scott, 1987). Teaching hospitals tend to be large and more capital intensive. Additionally, teaching hospitals treat more reliable complicated cases that have higher demand variability than non-teaching hospital. Therefore, reliable facility management measures should be incorporated into facility management decisions. The facility management focusing on patients’ expected length of stay and crucial decisions variables for effective facility management (Griffith et al., 1979; Flood and Scott, 1987). Teaching hospitals usually have full bed capacity due to the complex cases they treat. However, they may demand updated equipment and facilities. In relation to HGH which has a strong Saudi Board Program for Internal Medicine and this gives a good opportunity to deal with the medical cases they encounter based on Evidence-based medicine (EBM) or evidence-based practice (EBP). “It aims to apply the best available evidence gained from the scientific method to clinical decision making.[1] It seeks to assess the strength of evidence of the risks and benefits of treatments (including lack of treatment) and diagnostic tests (Wikipedia).
(Abernathy and Hershey, 1972; Cohen and Lee.1985; Erickson and Finkler.1985; Flood and Scott.1987; Smith-Daniels et al., 1988) suggest the demographic variables serve as the basis for health service capacity recourse management decisions.
H1a: The relative size of hospitals (number of beds) has a significant effect on hospital facility management decisions.
H1b: Hospitals geographic location (urban and rural) has a significant effect on hospital workforce decisions.
H1C: The medical education involvement of a hospital has a significant effect on hospital facility management decisions.
H1d: The medical education involvement of a hospital has a significant effect on hospital equipment/technology decisions.
Facility management decisions
Facility acquisition and utilization decision
Previous research on facility management decision in health care indicate that decision on facility acquisition and utilization could affect workforce and equipment/technology management as well as hospital cost and quality performance (Griffth et al.,1976; Smith-Daniel et al., 1988). Facility management is considered as the front end in a hospital resource needed to perform the various activities with right priority. According to (Barber, 1977; Hancock et. al., 1976; Lowery and martin, 1992) there are issues to be examined on facility management decision in each hospital. These are: in-patients admissions and surgical scheduling based on expected length and patient mix with place constraint on workforce and equipment decisions. For instance, bed capacity in HGH is an important problem.
For the decision makers it could be seen in two view, either it is caused by a disaster or expanding the mind for more solutions. Therefore, the hospital must provide Decision Making Strategy Utilizing Priority setting and program Data. The use of decision making theories and models has become increasingly popular since the mid-1950s. Various disciplines including economics, business management, psychology, and political science have proposed models and techniques designed to yield a systematic and rational decision making process (Graham W. Ward, Letter to the Editor, Journal of the American Medical Association 236(1976):1351). Decision making can be defined as “the process of choosing between alternate courses of action” (Qfinance Dictionary). The priority of an objective is set by the critical decision makers for a program: experts in the field, policymakers, or consumers. Database is as an organized collection of data for one or more purposes, usually in digital form. The first step in using the decision strategy is to involve the goals needed and prioritize them according to the data we acquired. The projects which were encountering HGH to be established and constructed are: Emergency and Inpatients bed capacity, Water tank, Physiotherapy expansion, Pharmacy expansion, Outpatient expansion, Medical Record expansion, Air condition infrastructure. These motivate HGH to think about its process of priority setting and program data.
Workforce management decisions
Staff mix and scheduling
An adequate staff mix and effective staff schedule are postulated to have direct impact on quality of service and the cost of service (Abernathy et al., Offensed, 1972;Siferd et al., 1994). Health care services require constant interaction with patients. In the healthcare industry, patients come randomly and require direct and promote services from healthcare providers. A good strategy for staff mix and their scheduling will facilitate time varying demand at the same time as improving the quality performance. In relation to Nursing affairs services in HGH which did a cross-training for all staff to overcome any shortage in any of the departments.
Workforce development
A more competent and knowledgeable staff is suggested to be more likely to design efficient processes and deliver services that meet customer needs and expectations (Quinn,1996; Sulek wt al., 1995).To maintain the quality performance in health care services, hospitals emphasize on human resources development. These activities according to (Award Criteria, 1995) include; improving work force flexibility, enhancing service innovation, and increasing workforce training. These actions were taken in HGH to implement the standards of JCI (Joint commission International Accreditation). The qualifications required each nurse to be registered and licensed.
The impact of hospital’s quality performance from program data on decision making
The hospital’s quality performance is linked by implementation of the high technology. Providing the hospital with data may vary from equipment to others which might have strong impact on patients’ services as well. In the 1970s, a new medical technology emerged. During the 1980s, acquisition of new major equipment was a critical decision regarding technological acquisition which was the amount a hospital should invest in clinical and administrative equipment/technology, and patient medical record information systems (Pegels and Rogers, 1988).In healthcare sector, clinical technology may increase expenditures since additional diagnostic and therapeutic procedures are made by advanced technology. In HGH there are some departments that used technology to improve their outcome such as Out-patients department by giving patients an electronic serial numbers to enter the clinic. Advanced and high technology equipment’s study is usually done by executive committee with concerned members to prioritize the departmental needs. It is impossible to provide each department with all new and equipment they need at one time.
Performance criteria
A comparison of performance data of competing hospitals in the same area, or other comparable hospitals demographics can be used to analyse relative hospital performance (Comparative Performance of US hospitals, 1993; The Guide. 1998). Cost and quality are the metrics used to measure performance. These measures may provide affordable quality health services for general public.
Cost measures
Healthcare care cost measurement usually focuses on holding down patients cost (Fetter et. al. 1980; Flood and Scott, 1987; Williams et. al. 1998), achieving high labour productivity (Siferd and Benton, 1994; Trivedi and Warner, 1976; Warner and Prawda, 1972), and maintaining higher capacity utilization levels (Hancock et al.1976) page 602 (L. Li, W.C. Benton/ European Journal of Operational Research 146(2003) 596- 614).
Quality measures
Quality measures usually include clinical quality and customer satisfaction (Li and Benton, 1996; Williams et al. 1998). The Clinical quality measurement includes appropriate equipment, timely treatment, adequate amount of services and meeting the acceptable standards of the industry’s practices. To have clear guidelines for customer needs, you must react to their requests and complaints by collecting and analysing them. The feedback could identify areas for improvement.
And is it possible to forecast future capacity management for sudden crises, particularly during the Umrah and Hajj season (crowded seasons)?
With reference to Delia 2007, it was mentioned that there was a plan for disaster surge capacity such as a building fire and a small airplane crash. They give clever suggestions to deal with such crises. They suggested tents, cafeterias, overflow areas. This is what we called as peak periods in our case study in HGH Ramadan and Hajj seasons. These are two events of great significance for Muslims. During each Hajj season, three to four million Muslims from all over the world will gather in the Holy city of Mecca to perform Hajj (pilgrimage). Thousands of people also visit Mecca throughout the year to perform Umrah (the lesser pilgrimage).
Research Methodology
What is Research Methodology?
When a student conducts a research, he is required to look at a company from a new perspective with considering the existing data to be investigated, evaluated and eventually given the organization benefits. Methodology is, broadly speaking, the way in which a researcher conducts research. It is the way in which he chooses to deal with a particular question (which may consequently result in a problem definition).Ref. Rene´ Descartes (1596–1650). It is a challenging chance for me to take the problem of Hera’a General Hospital and give a close study from a researcher’s point of view.
According to (Jan Jonker l Bartjan Pennink) research methodologies are “a way to conduct the research that is tailored to the research paradigm”. The aim of applied research is to provide solutions to problems that occur in practice. Researchers focus on creating (re)designs and plans of action for these problems. Most researchers are taught to deal with these problems during their studies by following a three-step approach: diagnosis, design and change. The diagnosis of HGH was an out-come of Team work group who notice, realize, and report. The resistance from some of the concerned staff to change is expected due to the alterations encountered during the implementation of the suggested new policy.
Defining Methodology.The word methodology is derived from the Greek ‘meta hodos’ meaning ‘the way along which’. In more everyday language it means ‘… a system of methods and principles for doing something’ (Collins Cobuild 1987). A methodology assumes there is a logical order the researcher needs to follow in order to achieve a certain predetermined result (e.g., knowledge, insight, design, intervention, change). The combination between quantitative and qualitative research might be used to produce outstanding results. The reader must realize the difference between both methods since Quantitative research is often regarded as being purely scientific, justifiable, and precise and based on facts often reflected in exact figures. Conversely, qualitative research is often regarded as ‘messing around’ being ‘vague’, not scientific and not following a structured plan. In my dissertation both were having clear touch in clarifying the study.
Research” Data Techniques”
Techniques for doing research indicate how the researcher can either think about his research or carry out specific actions in that research. Acting techniques are the researcher’s ‘tools’. They shape and guide the way in which data is generated, established, classified and analysed. Data is considered to be ‘raw’ information, usually in the form of facts or statistics that you can analyse, or that you can use to do further calculation (Collins Cobuild Dictionary 1987, p. 357). Or: facts (attitudes, behaviour, motivations, etc.) collected from respondents or observations (mechanical or direct) plus published information (Cooper and Schindler 2008, p. 82).
This data may be collected deliberately generated such as if the researcher prepared a questionnaire to have answer scores or data that already existed in the organization like annual reports for the last 5 years as what we had in this dissertation.Data can be classified based on its nature. A distinction can be made between linguistic data (e.g., transcription of a conversation), numerical (in figures) data (e.g., a company’s profit and loss account) and visual data (e.g., drawings, pictures, photos, rich pictures, etc.).
The researcher could translate the facts by focusing on the methodology and technical ‘translation’ of the problem into research instruments (techniques). The methodologies of research depend on the types of analysis that are intended. They use ethnography that aims to gather empirical data on social behaviour through several means. These are: interviews – where personal experiences are sought from selected individuals; focus groups – where a group’s belief is explored; conversational analysis –where personal nuances and expressions relay hidden information; and finally case studies – where historical evidences prove a point or practice (Lincoln and Guba 2000; Gephart 1999). Such studies help interpreters to uncover the socially constructed meanings that cannot be understood in the ordinary course of things. As opposed to positivists, interpreters do not accept the applicability of a universal law; rather, they discover how these laws are bypassed under diverse environments, and thus create research problems (Cavana et al 2001). In this research I used Case study followed by a structured and detailed interview as technical support needed. In this methodology the researcher will do nothing more than observing during or after certain events; the researcher is not able to intervene intentionally and to determine the possible effect of that intervention. In order to be able to make predictions about possible effects the researcher will need to compare his results. This remains a complicated and often biased affair. The researcher can choose between the possibilities such as a norm or another existing case or a theory.
The criticality of a research might indicate that both the qualitative and quantitative research approaches comprise a tremendous variety of requirements that are not always easily combined. Conducting accurate research based on one – or both – traditions is not simple. Combined with the demands of the internal or external client the researcher could soon find himself in a ‘methodological minefield’.
Research Design
This study aims to discover how HGH achieves its objective of having good utilization for its bed capacity through best used of quality tools for measurements of the organisation priorities and program data. It fits well into the interpretive paradigm, and a case study research method is most suitable for this effort (Lincoln and Guba 2000; Gephart 1999). As the research problem is mainly about “how” and “why”, a qualitative case study methodology can yield richer details of data not available through other research methodologies such as surveys (Eisenhardt 1989, Yin 1992). Moreover, a case study is especially appropriate for studying modern-day trends or conditions in a rapidly changing real-life situation where the place, period, people and process affects the trend or condition and vice versa, and when several sources of data are used (Yin 1994), as will be the case in the current study.
This study investigates the use of priority setting and program data in having best utilization for bed capacity in HGH. This entails bed allocation on the best basis, replacing the prevalent methods of first come first served, as well as overcrowding, as both tend to ignore trends and possibilities of fetching better returns. For this purpose, a study of current HGH capacity management which is considered the first pilot in the Saudi Healthcare, and also of New Jersey hospital in order to view comparative practices. A review of such cases will provide predictable similarities due to their common background and environment (Carson et al. 2001).
To answer the first phase of the research questions, the study will use a two stage approach to develop the data collection plan. The first stage will include a pilot case study that will be conducted to gather information in order to refine the data collection plan to gain better results in the subsequent cases. Secondary data such as books, journals and articles from libraries, and other relevant materials will be collected to aid the research. After conducting the pilot case, the interview data will be categorised and analysed. Upon completion of the formal data collection plan, the research will move on to stage two to study the other case. In stage two, the researcher proposes to collect in-depth interview data from Bed capacity management program members by following the formal data collection plan, and will employ a non-structured interviewing methodology with open-ended questions.
The data will be analysed in a systematic manner to see if the research questions have been answered, and whether the research objectives are substantiated. After preparing, indexing, organising and source coding the raw data collected, the researcher will interpret what has occurred by identifying the themes and sub-themes from the raw data collected. Content analysis will be used to identify themes by identifying, coding and categorising the primary patterns in the data collected. A constant comparative method will be used to compare and separate themes by reading the raw data. The researcher will also be able to recognize unique patterns of specific cases and formulate patterns across cases (Eisenhardt 1989). Through the use of structured and diverse view of the data, a generalised understanding, with supportive data, will be developed. The results will be presented and recommendations for further research, if required, will be offered at the end of the thesis.
Case Study of Hera’a General Hospital
The case study hospital capacity management chosen for this research is Hera’a General hospital.
HGH is a public sector hospital that was established in 1983. It employs approximately 2500 staff. The capacity bed started with 269 beds. The concept of Quality was initiated by the Medical Director in 1998 in the clinical areas during his monthly meetings. No Quality department had been established yet. That was when the concerned people who were calling for Quality were a doctor and a Quality assurance nurse who was hired on the 20th of July 2001. They did a tough job through holding lectures about quality awareness for the clinical departments. There was no standard to follow, so they just followed JCI (Joint Commission International) standard to be adopted by the local resources in order to develop the performance indicators. The single most important determinant of an organization’s success in implementing total quality management is its ability to translate, integrate and ultimately institutionalize TQM behaviours into everyday practice on the job. And, because of line management’s vital role in leading the organization, their ability to tangibly and consistently demonstrate their buy-in through their actions is particularly critical. It is not enough to any more be smart, hardworking, and able to show results – because nowadays everybody can do this. What really set an organization is how to make quality the responsibility of everybody in the organization. From 1998 up to 2003, we may seem to understand that the early diagnostic stage was not valid as the analysis of all system and processes were not activated. One the other hand, the statistical approach with the cooperation of the I.T. department was not there. The whole description and criticism of this duration could be under awareness, as the concept of quality costing and benchmarking was initiated.
According to J. Michael Crouch (1997) “the single most important determinant of an organization’s success in implementing total quality management is its ability to translate, integrate and ultimately institutionalize TQM behaviours into everyday practice on the job. And, because of line management’s vital role in leading the organization, their ability to tangibly and consistently demonstrate their buy-in through their actions is particularly critical.
In 2004 the philosophy of our organization moved to an extreme change in terms of quality. Management in its pursuits of quality improvement, customer satisfaction, and market share and profit enhancement uses quality costs as the economic common denominator, which forms the basic data for TQM. A quality cost program provides warning against upcoming dangerous financial situations. Quality costing is one measurement technique that has often been used to help justify the adoption of quality improvement efforts by senior managers (Sinclairet al., 2001). A number of world-class organizations do employ quality-costing measures as an indication of internal quality performance (Dale et al., 1999). According to Bester field (1994) “Quality costs are defined as those costs associated with the non-achievement of product or service quality as defined by the requirements established by the company and its contracts with customers and society”. Simply stated, it is the cost of poor products or services. Juran is often given credit for coining the concept of quality costs. He addressed the economics of quality in the first quality control handbook (1951) in which he used the famous analogy of “Gold in the Mine”.
In 2006 with the facts registered in our hospital about unnecessary lab investigations requested by the Emergency department, the printed forms, lab resources, manpower and waiting time of the patient cost the hospital much. The repeated complaints from the Laboratory staff regarding unjustified investigation encouraged top management to do a research about quality cost.
The committee assigned for this study proposed that an optimal quality level could be found where the losses due to defects were equal to the cost of quality control. The “cost of poor quality of an organization is the difference between the actual operating cost and what the operating cost would be if there were no failures in its system and no mistakes by its staff (Bland et al., 1998). They remarked that quality costs are a measure of costs specifically associated with the achievement or non-achievement of product or service requirements established by the organization and its contracts with customers and society. The process of internal and external failure costs, appraisal cost and improvement costs shows a great result in reducing the percentage of investigation used from 13% to 7%. The percentage of revenues in service exceeds 40 per cent due to the fast discharge of patients with higher level of satisfaction. This also gives a clue to the Top management to focus on a bed capacity management in ED and its consequence problems to be tackled. The hospital director conducted several meetings with senior managers and concerned staff from ED to discuss, evaluates, recommend and solve.
Quality is the choice
As we have noticed above, the initial phase of implementing TQM was done well through communication, and sessions done for the physicians in the orientation program. The awareness that imposing goals can be made achievable by means of innovative ideas can in itself be classified as a “mental” best practice, without which fundamental improvements are not possible. The commutation, coordination and commitment tools were the language of HGH staff in order to implement departmental and hospital strategy. The sessions that were made by TQM department have a great role in this effect through the activities that were made weekly, monthly and annually. The annual celebration of Quality Improvement Week gives the impression of great commitment to quality from everybody in the organization.
“The coordinating tool of implementation concerns more relevant organization and senior management structure” (TQM.MN7322/D©University of Leicester 2007p. 55). The department heads supported the hospital strategy by developing their policies and procedures and the tasks distributions of daily work to be as a guide for the staff at all times. The evaluation of Quality Management Program must be submitted to the top management to consider the success and failures of the implementation program.
The hospital now has a clear strategy built up by its Quality Council chaired by Hospital Director, who also chairs the other committees such as (Executive Committee, Supervisory Board, Resources Allocation Committee, etc…) to monitor the on-going implementation of the strategy and to build a system for its development. In our hospital the Multi-disciplinary Teams (Committees, Task forces, Quality Improvement Teams, etc.) with members from across all the departments is the responsibility of the Quality Administrative Coordinator. Monitoring the process and system is done through the analysis of and the reporting of minutes of meeting to the top management. In this practice this allows the improvement of an entire system by the coordinated efforts of all those working in the committees as members from the different departments involved (TQM.MN7322/D© University of Leicester 2007p. 59).The carefully selected members for these committees are like the facilitators who assists the organisations’ intention with regard to quality.
Utilizing Program data
HGH Priority setting criteria
The best utilization of data in HGH was done in the year of 2008 when the Hospital Director called for collecting data related to the projects. These projects are: Emergency and Inpatients bed capacity, water tank, physiotherapy expansion, pharmacy expansion, outpatient expansion, Medical Record expansion, Air condition infrastructure. HGH creates its priority setting criteria based on the following quality tools measurement. In carrying out quality improvement initiatives in the hospital, departments and teams should prioritize improvement activities that meet one or more of the following criteria:
- Alignment with MOH and Hospital mission, vision, values and strategic goals
- Meets the needs and expectations of internal and external customers
- High volume diagnoses/procedures/ and other operational and business processes; means (Is this project clearly associated with the mission of the organization?)
- High risk diagnoses/procedures and other operational and business processes; which means; (is the target for this project addressing an area that present a serious threat to patient)
- Problem prone diagnoses/procedures and other operational and business processes
- High cost diagnoses/procedures and other operational and business processes
- Meets Central Board (CBAHI) requirements
- Meets Joint Commission International (JCI) requirements
- Practices cost containment and effectiveness
The general criteria above were arguing the concerned decision makers in HGH due to the limitations in budget which is provided by Ministry of Health who they must be convinced by tangible facts and scientific view to give the financial support needed. The Hospital Director did extreme efforts for this issue and requested the ITD for needed Data to support his requirement of expensive projects below to meet the Minster of Health and took his approval for granting ED expansion with 11 million Saudi Riyals.
- Water tank
- Emergency
- A.C. Infrastructure
- Medical Records Expansion
- Out Patient Department expansion.
- Pharmacy expansion.
The below projects prioritization form declare the hospital systems in prioritizing the issues.
So from all listed projects the most important project is bed capacity management which presents the approval of ED expansion with 55 beds which was mainly the problem since it was with 23 beds. This decision was taken by concerned members in executive committee which is chaired by Hospital Director. The focus of Hera General Hospital on capacity management resource processes are such as: facilities; equipment and the workforce which are the main target to reach to the quality care and meet the customer needs.Comparing the situations of ED in HGH and New Jersey might give a clear view for the outcome result. Focusing on ED bed capacity might lead the administration to different recommendations which lead to effective and quality services. In response to concern about growing utilization of hospital emergency departments (ED’s) and its implications for hospital surge capacity, the New Jersey Department of Health and Senior Services (NJDHSS) commissioned the study “Emergency Department Utilization and Surge Capacity in New Jersey” to be conducted by the Rutgers Centre for State Health Policy (CSHP). Hera’a General hospital responded positively to the growing numbers of patients in ED and In-patients department. HGH examined the yearly occupancy rate, numbers of admissions and discharges in Emergency department and in-patients length of stays for those cases during 2004 up to 2008.
This data indicates that percentage in occupancy rate is increasing gradually. Overcrowded ED’s also create an environment where medical errors are more likely and overall quality of care is below its potential (JCAHO, 2004). Derek Delia (2007) declared that if you want to understand the multiple factors which help ED to provide services. Those factors have great influence in providing the required services for patients in ED department. The size of hospitals (number of beds) has a significant effect on hospital facility management decisions. The phenomenon of suburban sprawl may exacerbate the effects of population growth on ED crowding. Suburban growth is associated with increasing rates of automobile accidents, but ED and trauma care resources are typically insufficient in these areas and lag behind population growth (Millard, 2007). This places even greater demands on urban ED’s and trauma hospitals. In addition, hospital ED’s experience an increase in demand when a nearby hospital closes its ED or ceases operations altogether (Sun et al., 2006). In relation to our case study HGH is located in Mecca and it is registered with the highest population among all regions in all the kingdom of Saudi Arabia.
Hospitals geographic location (urban and rural) has a significant effect on hospital workforce decisions. HGH is in urban and ideal with many urban dwellers nearby in the north area of Mecca city which need to be supported by staff in all fields. The medical education involvement of a hospital has a significant effect on hospital facility management decisions. In teaching hospitals, ED throughput can be slowed down by the need to train residents in emergency medicine. It has been shown in other contexts that residents often generate inefficiencies by ordering more tests and processing patients more slowly than experienced physicians (Kuttner, 1999; DeLia, Duck, and Cantor, 2003). This may be especially problematic in the ED where the urgency of many conditions and the need to streamline patient flow require rapid decision making. Despite the inefficiencies, training the next generation physicians remains an important mission of teaching hospitals. As a result, there is a need to balance potentially conflicting goals of training and efficiency in the ED. The medical education involvement of a hospital has a significant effect on hospital equipment/technology decisions.
Measurement of ED Overcrowding
Although the problem has been well documented, rigorous measures of ED overcrowding are not fully developed and universally available for research and evaluation. At issue is the reliability of overcrowding measures across facilities and regulatory jurisdictions. For example, ambulance diversion is often taken as a sign of an overcrowded ED. However, hospitals have different criteria for going on divert status. In some parts of the nation, hospitals can divert ambulances simply to avoid additional patients that have been diverted from other hospitals in an apparent gaming of the system (IOM, 2006). Other crowding indicators such as “excessive waiting times” also suffer from lack of standardization. To generate consensus and standardization of ED overcrowding measures, Solberg et al. (2003) received funding from the federal Agency for Healthcare Quality and Research (AHRQ) to convene an expert panel who reviewed a list of 113 potential measures. Using the input/throughput/output framework described above, the authors narrowed the original list to 38 measures (15 inputs, 9 throughputs, and 14 outputs).
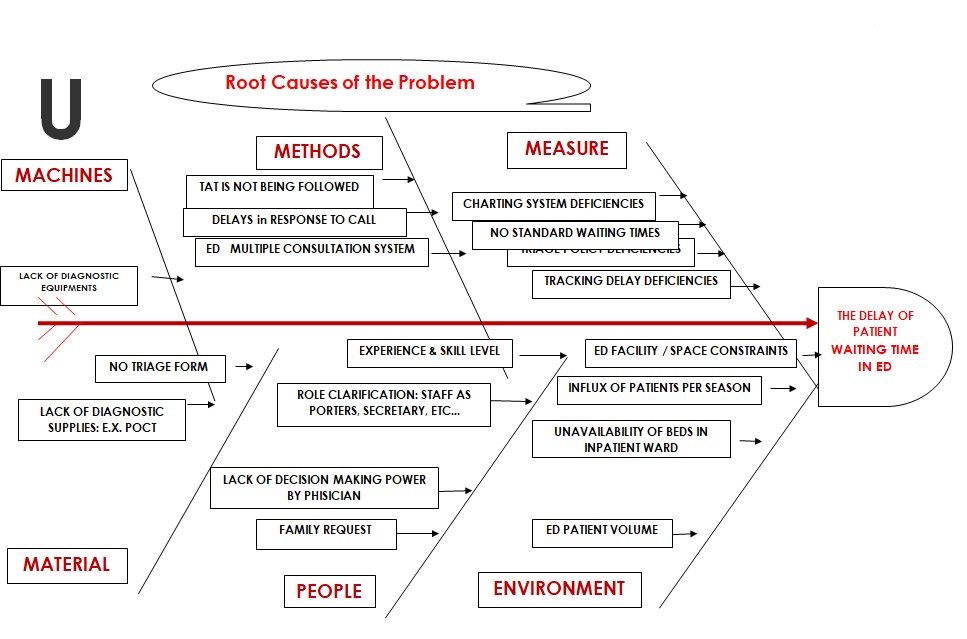
Some of these measures such as hospital census and occupancy rates can be calculated with existing administrative databases. Many others require much more detailed data about hospital processes. Examples include; patient waiting time from registration to provider contact, EMS waiting time at the hospital, and the ED occupancy rate defined as the number of registered ED patients divided by the number of staffed treatment areas at a specific point in time. The quality culture of HGH was a guide to discuss problems in the organisation’s atmosphere. One example showed in the nursing implication on the delay of patient waiting time in Emergency Department. The study is based on the quality tools to measure the reasons of the problem. The quality department in HGH has participated in studying departmental problems and guides them to the target need. The study showed in details below the efforts done by Nursing Services department. The Quality Improvement Methodology for conducting study in HGH is FOCUS-PDCA. The meanings of these abbreviations are:
Quality Improvement (QI) study application form
Which priority setting criteria does the subject or the study/activity meet?
- High risk
- problem prone
- Internal and/or external customer satisfaction √ Cost containment
- MOH standards requirements
- Accrediting body requirements
Objectives
Department/ team involved
Resources needed: (information, staff, financial, time, etc.)
Does the study have any impact on the following QI outcomes of care/services?
What is the impact of the study on patient care delivery?
FOCUS-PDCA Methodology in conducting the study
| F | Find – an opportunity for improvement
According to a report in the November 9 issue of Archives of Internal Medicine, one of the JAMA/Archives journals, : ” Prolonged emergency department (ED) wait time decreases patient satisfaction, limits access, increases the number of patients who leave before being seen and is associated with clinically significant delays in care for patients with pneumonia, cardiac symptoms and abdominal pain,”. |
 | |
FOCUS-PDCA Methodology in conducting the study
Measurement of Patient Flow
According to (Derek Delia 2007) in his case study he mentioned that “For some hospitals, the alleviation of overcrowding may involve additional capacity staffing, or physical space”. However, there is a well-developed school of thought, which argues that these extensive and generally costly approaches should not be tried until a hospital has fully evaluated and optimized the flow of patients though the ED and related units. “This school emphasizes that adding new capacity to an inefficient system may just create larger facilities that remain overcrowded” (Derek Delia 2007). This situation is similar to what happened in HGH when they finished the expansion of ED. they thought the problem had been solved while in fact it created other situational crises related to Bed management in the in-patients departments. Since HGH is one among 10 hospitals which are involved in JCI (Joint commission International Accreditation), there were instructions to promote patients flow by the guidance of JCI workshops related to this subject. In New Jersey many other strategies focus on improving ED output by streamlining patient flow in other units of the hospital.
This may be done through coordinated bed management where a “bed czar” or patient flow team constantly monitors the flow of patients through all units of the hospital. HGH has established discharge planning office to monitor the status of bed during the day. It has as well established the new Bed Management Program to deal with its problems related as it was initially suggested for the hospital. This program is defined as: A program that assists a patient to get a bed in addition to follow up, develop and evaluate the performance of ministry hospitals in this aspect. We must highlight that this program is connected to all hospitals in KSA. The vision of this program is to make a bed easily available in routine and emergencies. The mission is: Optimal use of available resources to ensure effective and efficient use of beds. The values are: Teamwork, Justice, consideration of patient’s rights, efficiency and effectiveness, transparency, improvement and development. The general objective of this program is; to ensure management and operation of beds efficiently and effectively shorten the length of stay and increase the bed turnover to provide beds for patients in routine and emergencies. The approved program with guidelines for the concerned members is attached (appendix C).
Data Analysis
Analysis
This section of the dissertation provides analysis of bed capacity for our case study HGH. The trends in occupancy rate, admission, discharge, average Length of Stay for (In-patients) departments in HGH are analysed. Then the numbers of patients and average of waiting time per minute in Emergency Department is also analysed. Data is obtained from the Hospital Information System (HIS) from 2004 to 2008. Due to limitations in data availability, analysis of patients who were treated and released from the ED is restricted to 2004 to 2008. This section concludes with brief analysis of population in Kingdom of Saudi Arabia for the main cities.
Annual trends
After rising steadily in numbers of patients from 2004 to 2008, total admissions in HGH fell slightly in 2008 (Figure 2).In 2007, the admissions represent the highest annual volume of admissions for the study period. The reasons of such variation will be mentioned below.
The increased numbers of patients from 2004 to 2007 is considered to be normal. In contrary, the decreased percentage in 2008 by 5% compared to 2007 revealed that there must be defect in year 2008 since the percentage of patients who are in ED waiting for admissions are increasing in the same year which will be explained later.
Since the total of discharged patients varies by year, figure 3 shows the change in these numbers. We may notice that the least numbers of discharges matched with the admissions was in 2007. There were 617 patients who were not discharged in the same year. While the highest discharge was in 2008 which justifies the low percentage of admission in 2008 since there were admitted patients for 2007. These all affect the percentage of occupancy rate and the best utilization of bed by the concerned medical team.
The bed occupancy rate generally rose from 2004 to 2008 reflecting the longer term trend among hospitals nationwide to operate with less excess capacity. According to study into” Hospital capacity, Patient Flow, and Emergency Department Use in New Jersey” by Derek Delia (2007) “that occupancy rate above 85% may raise concern about capacity constraints”. Occupancy of 75% is well under this benchmark. HGH faced similar experience as shown above; the occupancy rate was increased from 2004 to 2007 and decreased in 2008. The occupancy rate might be affected by the numbers of admission and length of stay. The importance of having less average of length of stay compared to highest numbers of patients to have ideal occupancy rate which reflects best bed utilization required be the leaders in healthcare field.
This variation in length of stay may show the reason of defects in the decreased numbers of admissions for patients in figure 2. The length of stay is increased in 2008 which affects the admission in the same year. The only justification for this is the lack of implementing the discharge plan by the medical team according to the diagnoses. The lack of implementing and activating the role of each member in the medical team leads to delay in discharge and admission accordingly. The medical cases which record high length of stay are: Cerebral palsy, Cardiomyopathy and Respiratory failure.
The target for this census is to show facts and help the administration to deal with it accordingly. In ED department the data shown below is reflecting the highest increase of numbers of patients from 2004 to 2008 and average of waiting time as well.
Providing the above data for ED department, it shows the increased numbers of patients from 2005 to 2008 by 39%. Then, in the latest two years the percentage increased by 1.8% which means good utilization for bed capacity.
The average of waiting time is balanced with numbers of patients which is logic due to the increased numbers of patients. In recent years, the ED has grown in importance of in-patients admissions to Hera’a General Hospital. The data showed a great interest to evaluate the situation and ask the higher authority to expand ED to accommodate all patients arrived in ED. The project costs 11 million SR.
Findings
This section summarizes findings from the case study analysis. The goal of the analysis is to understand sources of stress on hospital bed capacity in ED, how hospitals manage patient flow through the ED and other units, potential barriers to implementing best practices, how hospitals coordinate care with primary health centres and implications for surge capacity. The case studies consist of telephone interviews lasting approximately 30 minutes with key in informants from departments in HGH. Informants include departmental heads, ED director/doctors, nurse managers, and discharge planning officer. A copy of the interview protocol is found in the Appendix.
In-patients and ED departments were chosen based on occupancy rate in HGH. The original design envisioned matched pairs of hospitals that are similar in occupancy rate. The table below declared the highest occupancy rate recorded for HGH among all hospitals in Mecca.
Figure: Comparison of HGH for total beds, admissions and occupancy rate.
HGH is experiencing high increased numbers in admissions, discharges and occupancy rate compared with other hospitals which are experiencing little occupancy rate. The implementation of required process for activating the best utilization for bed capacity was not as expected. Moreover, interviews were conducted with concerned members from different departments of HGH that have in their overall occupancy rate but are not considered matched pairs. The yearly data of occupancy rate is based on data from the hospital system analysed above as well as from direct questioning of interviewees. The data indicated during the interview that they were having serious problem in bed utilization which caused high occupancy rate per year.
Compared to Mecca hospitals, our case study Hera General Hospital operates at higher occupancy, and more likely to be members of teaching hospitals. HGH covers a wide range of areas across Mecca city. In these particular characteristics HGH is facing similar situation to what was happening in New Jersey. Some of the characteristics which are studies in both hospitals are; average numbers of maintained beds and average of occupancy rate.
Overcrowding and patients flow
In reference to Derek Delia 2007 case study, there was no overlap in the indicators that hospitals used to define and measure overcrowded condition. Hospitals might think of specific criteria involving cycle times for beds and laboratory tests. Another hospital defines ED overcrowding as a situation where at least 6 patients are waiting for care. This leads to serious question about hospital measurement on overcrowding. Each hospital could have its own measuring tool but it must be refereed to quality basis measurements either locally or international bodies measures such as CBAHI and JCI. The most common measurements to have been used in HGH and New Jersey hospitals are volume, occupancy, and patient acuity.
Three informants provided additional detail about circumstances where they have to give priority to high risk cases such as life threatening cases and they must accept any patients who came via ambulance. Although this might be adding load to the capacity since HGH did not have the specialty of RTA related. Ultimately, HGH refereed such cases to the hospitals which could be the suitable care for these cases.
Other informants declared that about 60% of ED cases are considered as cold cases and could be treated in the primary healthcare centres. Similarly, NJ and HGH informants had encountered same situation about the need for coordination with primary healthcare centres which was lacking. In all means, this large numbers were wasting the hospital resources for laboratory investigations and x-rays requests as well as increase the medical errors due to the increased of work for the ED staff. All departmental informants agree that better management of patient flow is crucial to have best utilization for bed capacity management.
The facilities were experienced by HGH which results to little overcrowding of patients by implementing discharge plan from date of admission of the in-patients’ department as well as implementing the bed management program mentioned above. Moreover, the activation of the Triage system in Emergency department was another suggestion to decrease overcrowding. That system help to filter cold cases and discharge them immediately and this was affecting positively in the length of stay data of the ED especially after the expansion of Emergency Department. In case for admitting more patients through ED, the load will be more for In-patients department. The incompliance to discharge plan policy by some of doctors was one of the reasons for delaying discharge of patients. Some doctors justify their delays for their commitments of covering the clinic in Out-Patients Department or performing surgeries during the morning shifts.
Hospital occupancy and capacity
The analysis above highlights the issues that are critical to distribution of hospital capacity in HGH. It is important to mention that Delia 2007 introduced in his study that this topic was underscored by the creation of the Commission of Rationalizing Healthcare Resources by Governor Corzine. In relation to HGH experience, I agree with the argument of (Delia,2006-b) in his study about the comparative case study in NJ hospitals that annual bed and utilization statistics give a misleading picture of the alignment between supply and demand for hospitals services. Participants in our case study declared that staffing shortage play an important role in the hospital care and quality services needed for patients. Emergency department was in need for more staff in all categories to support the additional bed added. The qualifications for ED staff are highly standards by the JCI accreditation due to the critical area they are covering. HGH did not have specific staff for triage area to deal with non-emergent cases and routinely refer patients to outpatients department. They are actually ED staff.
During peak periods, hospital capacity in all Mecca should be increased and supported to accommodate the huge numbers of pilgrims who are coming during Ramadan and Hajj season. Ultimately, most of those visitors need healthcare support. Under the directions of the Custodian of the Two Holy Mosques, King Abdullah Bin Abdul Aziz, of providing the best health services to the pilgrims in addition to Ministry Of Health efforts to maintain the pilgrims’ health and safety. Dr. AL Rabeeah notified that MOH asked 135 consultants in different fields to participate in providing specialized health services to the pilgrims and 24-hour cardiac catheterization and dialysis units. He added that the Ministry has implemented a number of new and developmental projects in various Hajj locations especially in the holy places that contain millions of pilgrims in a limited area. The Ministry of Health Planning and Development Deputy, Hajj Preparation Committee Chief, Dr. Mohammad bin Hamza Khusheim, has clarified that the developmental projects this year includes establishing a new emergency facility in Hera General Hospital with a capacity of 55 beds at a total cost of 11 million SR and its intensive care unit, replacing the infra-structure of Noor Specialized Hospital at a total cost of 120 million and develop and prepare its operation rooms at a total cost of 40 million, opening a daily treatment unit in King Abdul Aziz Hospital with capacity of 26 beds at a total cost of 6 million SR. On the other hand, the implemented health projects in the holy places this year included replacing and establishing primary health care directorate facility at Arafat and other health care facilities at a total cost of 3 million SR.
Moreover, Dr. Khusheim stated that the amount of the Ministry’s health care facilities is about 24 hospitals; 7 hospitals in Makkah, 10 hospitals in Madina, 4 hospitals in Mina and 3 hospitals in Arafat with a total capacity of 4005 beds. It is possible to deal with sudden crises capacity management particularly during the Umrah and Hajj season (crowded / peak seasons) if you have good strategy and leadership to support your decisions. This strategy should be ready for each hospital encountering pilgrims. Sudden crises are meant if huge numbers of accidents come suddenly or transferring of patients from the holy mosque due to the limited numbers of hospitals there. The management of for bed capacity in HGH faced this fact one day when they received 60 patients who were having poising. The reaction of HGH was to utilize the OPD waiting area and prepare it with beds to deal with the cases.
Conclusion
I believe that each author has put his imprint in the Quality world. I wish to be one of them one day. Deming (1982, 1986) “underlined the use of statistical techniques for quality control, and proposed his 14 principles to improve quality in organizations, based on the following ideas: leadership, an improvement philosophy, the right production from the beginning, training for managers and employees, internal communication aimed at the elimination of obstacles for cooperation and the suppression of quantitative objectives”. Juran (1986) pointed out the importance of both technical and managerial aspects, and identified the three basic functions of the quality management process: “planning, organization and control, as the stages for quality improvement; he indicated that the aim of the management is to reduce the cost of mistakes, reaching a point where the total costs of quality are minimal” (Juran and Gryna, 1993).
On the other hand, Ishikawa (1976, 1985) emphasized the importance of training, the usage of cause-effect diagrams for problem solving, and quality circles as a way to achieve continuous improvement. Crosby (1979) defined 14 steps for quality improvement, including top and intermediate management commitment, quality measurement, evaluation of quality costs, corrective action, training, a zero-defect philosophy, objective setting and employee recognition. Lastly, Feigenbaum (1991) “described the notion of total quality, based mainly on leadership and an understanding of the aspects of quality improvement, a commitment to incorporate quality in the firm’s practices, and the participation of the entire workforce, the objective being the reduction of total quality costs”.
The accomplishment of the Saudi hospitals services is measured by its obtained quality prizes and accreditation bodies as to whether it is locally by achieving internal accreditation such as CBAHI (Central Board for Accreditation of Healthcare Institutions) as well as further international accreditation such as JCI (Joint Commission International).
Nowadays, hospitals are seeking to have JCI which enhance the services for providing patient care in a newly competitive environment. The Joint Commission International (JCI) accreditation and certification is the proven process your organization needs to help ensure a safe environment for your patients, staff and visitors. This voluntary process shows your organization’s commitment to continuously improving patient safety. JCI’s members are dedicated to helping international health care organizations, public health agencies, and ministries of health evaluate in order to improve and demonstrate the quality of patient care while accommodating any specific legal, religious and cultural factors within a country.
Hospital capacity management should be given higher priority in evaluating the performance of the hospital in any community. The commencement of this dissertation was faced some obstacles as our country has no research related to be followed or at least to adjust to the current situation. I may criticize this for the lack of professional healthcare research centres which might support the organizations’ problems.
HGH’s bed capacity management was one of the main projects which were selected to be considered by the leadership. There were many reasons for delays such as limited space of the ED, lack of compliance of policy and procedures by the concerned members in HGH. Monthly statistics report and program data were strategies which assisted the decision makers in having straight decision of formation of the Bed Utilization Program and appointment of Discharge Planning Officer. The key indicators of HGH are hospital information technology Department statistics and workforce competence and these considered as the guidance to take actions by the decisions makers. Trends in the In-patients and Emergency Departments are heavily influenced by the inability of patients to gain access to primary and other specialized care. The facility management decisions in each hospital are the main targets to study discuss and solve on daily basis. HGH creates its priority setting criteria based on the quality tools measurements and the results came to highlight the need for expanding the location of ED department in new building with complete facilities. Ramadan and Hajj seasons are the two events of great significance for Muslims. Moreover, it is considered as peak periods in our case study in HGH for directors who care and plan for risk management in their organizations.
Using the quality tools in daily practice in hospital process was the clear guide for HGH to discover the problem and study the alternative solutions. FOCUS-PDCA was one of the quality methodologies mostly used tool for conducting most of the studies needed. It was used to evaluate and measure the waiting time in ED. The decision of expanding the location of ED was not the result of that study whereas utilizing the existing resources was the thinking of Nursing Director since the approval of establishing the new ED building was in process. Cooperation and activation of the Multi-Disciplinary Team Approach with the concerned departments was suggested to decrease patient stay delay in ED. In additional, the best use of Annual Evaluation of standard waiting times and its applicability and effectively rate in ED’s new as well as conducting Patient Satisfaction Survey annually specifically with regard to waiting times. The medical team should respond immediately to bleep. In relation to the advice to be given to healthcare institutions in relation to the bed capacity management program is the activation and compliance to the hospital policy.
Overall HGH experience was the answer for any persons why quality was the correct choice of leadership and every member of the organization.
Reference List
Al-Assaf (1998), Managed Care Quality, CRC Press LLC. Library of Congress –in-Publication Data. Page 31.
Ali Kokangul (2008). A combination of deterministic stochastic approaches to optimize bed capacity in hospital unit, Elsevier Ireland Ltd.
Beiman, L. Friedman, J. Olshen, R. & Stone, C. (1984). Classification and regression tree, California: Wadsworth International Group.
Brackett, M.H. (2001). Business Intelligence value chain, DM Review, Vol. 1(6), Web.
Business Dictionary. (2011). Capacity Management. Web.
Dara Sl, Shton RW.Famer JC, et al (2005) Worldwide disaster medical response: an historical perspective.Crit Care Med. P.33:S2-S6.
DeLia, D. Emergency Department Utilization and Surge Capacity in New Jersey, 1998- 2003. Report to the New Jersey Department of Health and Senior Services.
DeLia D. “Annual Bed Statistics Give Misleading Picture of Hospital Surge Capacity”. Annals of Emergency Medicine, 48(4): 384-388, 2006-b.
Derek Delia (2007), “Hospital Capacity, Patient Flow, and Emergency Department Use in New jersey”.
James E.McGown, Jonathon D Truwit , Pam Ciprian ,R Edward Howell, Margaret Van Bree, Arthur Garson , John Hanks (2007) Operating Room Efficiency and hospital Capacity: Factors affecting Operating Room Use During Maximum Hospital Census.
JCAHO. Joint Commission Resources. Managing Patient Flow: Strategies and Solutions for Addressing Hospital Overcrowding. Oakbrook Terrace, IL: Joint Commission on Accreditation of Healthcare organizations, 2004.
Ishikawa, K., 1985.What Is Total Quality Control? The Japanese Way. Englewood Cliffs, New Jersey, Prentice- Hall.
J.M.Nguyen,P..Six.D.Antonioli , P.Glemain, G.Potel, P.Lombrial , P.Le. Beux ,(2005) A simple method to optimize hospital capacity, Int, J,Med. Informed 74,39-49.
J.K.Cochran, A. Bharti( 2006) A multi-stage stochastic methodology for whole hospital bed planning under peak loading, Int,Ind.Sys,.Eng.1 8-36.
Jan ,Pennink (2010), The Essence of Research Methodology, Springer-Verlag Berlin Heidelberg Jee-In Hwang(2006) The relationship between hospital capacity characteristics and emergency department volumes in Korea.
Juran, J.M., (1951). Quality Control Handbook.
Ling Li, W.C Benton (2002), “Hospital Capacity management decisions: Emphasis on cost control and quality enhancement”.
J. Michael Crouch 1997 (1997, What You Can Do To Improve Quality. Web.
Li, X., Benton W.C., Leong K,(2002) The impact of strategic operations management decisions on community hospital performance. Journal of Operations Management 20 (4),389-408.
Millard W. “Suburban Sprawl: Where Does Emergency Medicine Fit on the Map?”. Annals of Emergency Medicine, 49(1): 71-74, 2007.
Orion.(2002) Bed Infection and Management Control. Web.
Peter Mears (1995), Quality Improvement Tools & Techniques, Library of Congress –in-Publication Data.
Robert Kanter ,John Moran(2007) Hospital Emergency Surge Capacity: An Empiric New York Statewide Study.
Ruth Hemphill , Bill Nole.Tulsa, Olka(2005) Relieving an Overcrowded ED and Increasing Capacity for Regional Transfers: One Hospital’s Bed Management Strategies.
Seung-Chul Kim, Ira Horowtiz, Karl K. Young, Thomas A.Buckley (1999) Analysis of capacity management of the intensive care unit in a hospital.
University of Leicester,(2007).What is Total Quality Management, University of Leicester 2007,p1.5), Learning Resources , England.
Witten, Ian H. and Frank, E. (2005). Data Mining: Practical Machine Learning Tools and Techniques, Morgan Kaufmann Publishers, San Francisco. Web.